Historically, medicine has treated neurodegenerative disease and cancer as opposite problems.
In conditions such as Alzheimer’s disease, ALS, and frontotemporal dementia, cells die too soon; in cancer, cells refuse to die — and grow out of control.
These appear to be opposite biological problems. (At first glance, anyway.)
But… researchers are increasingly discovering that diseases we once thought were unrelated may actually have similar explanations — or even the same underlying cellular vulnerabilities.
New research from Houston Methodist suggests that these two “opposites” — dementia and cancer — may share a common root.
The factor being singled out is a protein called “TDP-43.”
For years, researchers have recognized abnormal TDP‑43 accumulation as a major pathological feature in ALS and frontotemporal dementia —
…though its exact role in disease progression has remained unclear.
Suffice it to say that, if doctors find it clumped up in the wrong place in the brain, it’s interpreted as a sign of impending trouble.
But we didn’t have a clear picture of why it was there or what it was actually doing.
As it turns out, this protein appears to play an important supervisory role in how our bodies repair DNA damage.
Today, we’re going to look at how a “glitch” with this one protein “supervisor” can contribute to the breakdown of the brain on one hand, or to the growth of a tumor on the other.
[Video placeholder]
To understand this TDP business, we need to talk about how your body handles its “instruction manual” — your DNA.
Every time your cells divide, they have to copy billions of lines of genetic code. It’s like a clerk typing out a massive book by hand. Inevitably, the clerk is going to make typos. You might get an “A” where there should be a “T.”
Healthy bodies have a “Proofreading System” (scientifically called Mismatch Repair).
Technically, “proofreading” happens during replication in real-time; whereas, mismatch repair is a sort of after-the-fact damage control.
But, in general, this system scans the code, finds the typos, and swaps them out for the right DNA “letters.”
TDP-43 appears to help regulate parts of that proofreading system.
It doesn’t just do the proofreading; it helps coordinate when repair processes activate and how they function. When this system is balanced, your DNA stays more stable.
But the Houston Methodist study found that when TDP-43 becomes dysregulated, the whole system can begin to break down.
Let’s look at this a little more closely.
ALS and FTD
What actually happens in the brain?
Scientists have discussed two cases. The fits concerns the neurodegenerative motor-neuron disease known as amyotrophic lateral sclerosis, “ALS,” or — as I grew up hearing about it — “Lou Gehrig’s disease.” The second case study is frontotemporal dementia, or “FTD” — the latter has been in the news over the last few years due to the tragic diagnosis of famed Hollywood actor Bruce Willis, as we have discussed in other material. [Insert appropriate link(s).]
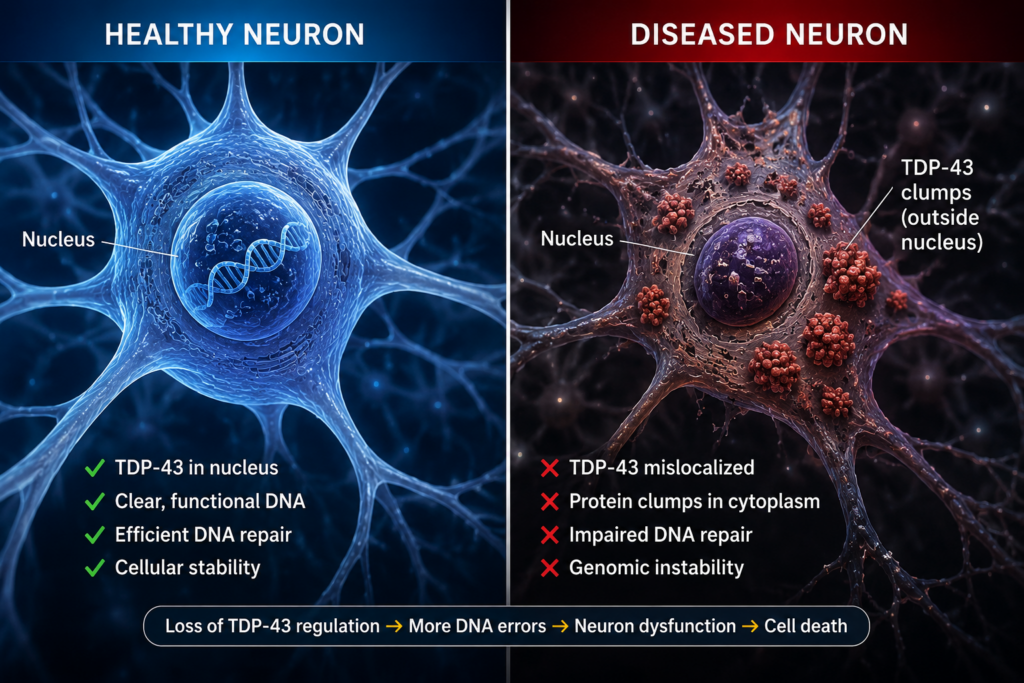
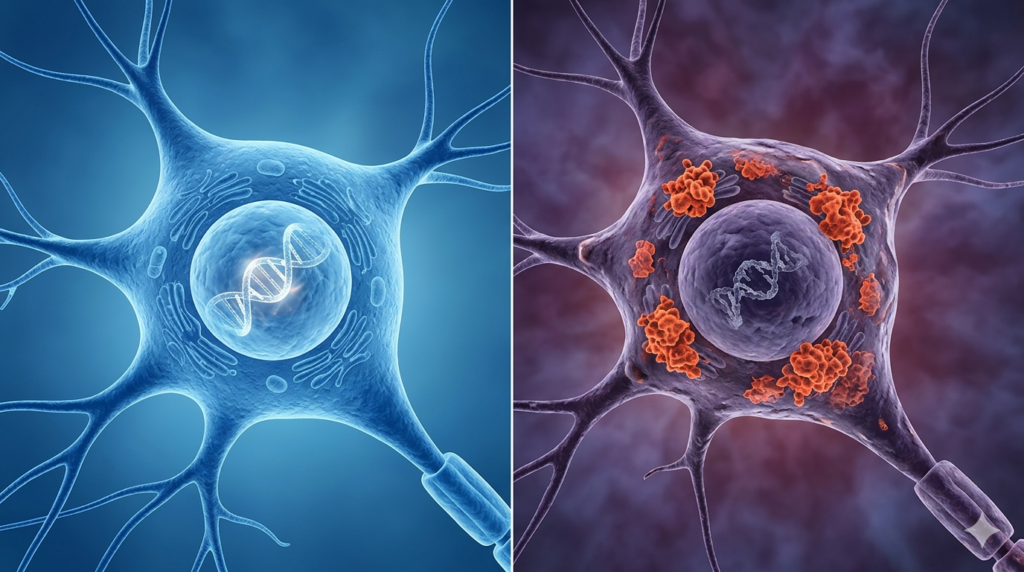
TDP-43 functions as a kind of DNA “Manager.” But, in ALS and FTD this Manager malfunctions.
It stops being where it’s supposed to be (namely, within the nucleus) and it starts clumping together in the “hallways” of the cell. This is the “Missing-Manager” scenario.
When the “manager” is missing or displaced, the repair system can become less coordinated and less reliable. This may allow more errors than usual to creep in, and for instability to build up over time — which, in turn, renders the neuron’s DNA volatile.
Over time, the cell can’t function because its “instructions” are full of errors.
Eventually, the cell gives up and dies. This mass “cell death” is what causes the symptoms of dementia — memory loss, loss of motor skills, and overall cognitive decline.
Now, let’s look at another side of the TDP-43 problem.
Cancer
Cancer is, at its core, a disease of corrupted instructions. Mutations can push cells to keep dividing, to ignore normal limits, and to survive when they shouldn’t.
The Houston Methodist team looked at large databases of cancer patients and found something striking: in many tumors, there is an over-abundance of TDP-43.
Call this the “Manager-in-Overdrive” scenario.
When there is too much TDP-43, the proofreading department may become imbalanced. This loss of equilibrium can — once again — allow genetic errors to accumulate more rapidly.
By looking at these tumors, researchers found that high levels of TDP-43 were associated with a higher “mutational burden” in multiple cancer types.
This basically means that a particular cancer is changing and evolving quickly.
Tumors with high mutation rates can become harder to treat because they may evolve in such a way as to develop resistance to chemotherapy or to evade the body’s immune responses.
So, while too little TDP-43 may contribute to the death of brain cells, abnormally high TDP-43 activity may contribute to tumors growing faster and becoming harder to treat.
This might sound like a “lose-lose” situation, but for scientists, this is actually an incredible opportunity. Before this discovery, we were trying to fix dementia and cancer using completely different tools.
Now that we know (or, at least, highly suspect) that TDP-43 and DNA repair may sit near the center of both processes, we have a potentially unified experimental target.
The findings suggest that restoring balance to these repair pathways could become a future therapeutic strategy. The aim would be to maintain TDP-43 in a sort of “Goldilocks zone”: not too much, not too little.
In the brain, this could mean protecting neurons by helping keep their DNA stable.
In cancer, this could mean slowing down the tumor’s ability to mutate, potentially making it easier to treat or more susceptible to a range of traditional therapies.
Caveats and Disclaimers
It’s important to note that this research is still in an early stage, and it’s focused primarily on understanding the underlying biology rather than testing new treatments in patients.
Additionally, both “cancer” and “dementia” are generic terms. This is to say that they range over an assortment of discrete — and, often, highly varied — conditions.
To put it another way, neither “cancer” nor “dementia” is just one, single condition.
Therefore, even if this TDP‑43 mechanism does prove important in — say — ALS and FTD, it does not automatically follow that it explains other dementias, including Alzheimer’s disease.
That said, we are starting to see the beginning of “cross-over” medicine.
Scientists are now looking at whether certain drugs used in cancer research could eventually be modified to help dementia patients — or vice versa.
The big takeaway here is that our bodies are incredibly interconnected.
A protein that we thought only mattered for brain health turns out to be deeply involved in protecting the integrity of our genetic code.
By understanding how TDP‑43 helps regulate DNA repair, researchers may eventually develop treatments that target deeper cellular mechanisms rather than addressing symptoms alone.
Eventually, we may learn how to restore balance to the dysfunctional systems that could be at the center of both cancer and dementia.
The lesson may not be that TDP-43 is “good” or “bad.” Rather, it’s that our biology appears to require a very narrow balance.
Too little may destabilize DNA repair in one direction. Too much may destabilize it in another.
It’s a reminder that in biology — as with a lot of other things in life — balance can be key.
Now, there are plenty of details that I have ignored. And, frankly, many of them may be beyond my ken. But if you want to dive deeper into the technical specifics of the study — I’ve linked the full article from the journal Nucleic Acids Research in the description below.
As a reminder, this channel is mainly focused on the health and science topics relevant for Alzheimer’s Proofing your diet, lifestyle, and — for caregivers — your home environment.
And on that note, I wish you all the best in whatever scenario you find yourself.
Thanks for reading! Don’t forget to check out the YouTube version!
Sources
Vincent E Provasek, Albino Bacolla, Suganya Rangaswamy, Manohar Kodavati, Joy Mitra, Issa O Yusuf, Vikas H Malojirao, Velmarini Vasquez, Gavin W Britz, Guo-Min Li, Zuoshang Xu, Sankar Mitra, Ralph M Garruto, John A Tainer and Muralidhar L Hegde, “RNA/DNA-Binding Protein TDP-43 Regulates DNA-Mismatch-Repair-Genes With Implications for Genome Stability,” Nucleic Acids Research, vol. 53, no. 18, Sept. 23, 2025 [online], Oct 2025 [print], <https://academic.oup.com/nar/article/53/18/gkaf920/8262242> and <https://pubmed.ncbi.nlm.nih.gov/40985771/>.
If you walk into any health food store today, you’ll see aisles dedicated to Omega-3 supplements. They’re sold as ‘brain insurance’ — the idea that a few capsules a day can shield you from Alzheimer’s, or other forms of cognitive decline and dementia.
It’s a multi-billion-dollar industry built on a foundation of some admittedly promising science. But lately, the narrative has started to shift. We’re seeing large-scale meta-analyses that don’t quite back up the hype. “Meta-analyses” are large studies that combine many clinical trials.
A few recent studies suggest we might actually be taking risks that we didn’t “sign up” for.
Today, I want to walk through some of the actual data — looking at four major clinical reviews, and one specific warning — to get a better handle on whether fish oil is actually protecting our brains, or if you’re just wasting our money on (potentially rancid) piscine oil.
This isn’t medical advice — just a look at what the current evidence actually says.
The Core Theory: Why We Care About DHA
To understand why we’re even talking about this, we have to look at what your brain is made of.
About 60% of your gray matter is fat — by dry weight. And a huge portion of that is a specific Omega-3 fatty acid called docosahexaenoic (/duh-KOH-suh hek-suh-NOH-ick/) acid, or “DHA.”
Think of DHA as a key structural and functional component of neuronal membranes.
According to a 2018 update on Omega-3s and Alzheimer’s [Source 3], these fats do two main things.
Firstly, they keep your cell membranes fluid. These membranes have to be flexible to stay functional when it comes to immune response, nerve signaling, and nutrient transport.
And, secondly, DHA fats act as powerful anti-inflammatories.
Early on, Alzheimer’s is often described as ‘low-grade’ inflammation — like a fire smoldering under the surface. But over time, that can escalate into something sustained and destructive that doesn’t fully resolve..
On paper, Omega-3s should help calm that process.
And, in laboratory and animal studies, Omega-3 has been shown to reduce amyloid-beta accumulation — the plaques long considered hallmarks of the disease.
Though, as we’ll explore in a future video, it’s worth noting that the amyloid hypothesis itself has taken some serious hits recently, including high-profile controversies over foundational research. The science isn’t as settled as supplement labels would have you believe.
And, as we’ve learned in medicine, what happens in a petri dish doesn’t always happen in a human being. Indeed, the “low-grade” label is increasingly being considered an oversimplification.
That said, none of this has stopped supplement suppliers from making promises about fish oil — promises that, as we’ll see, the clinical data doesn’t fully back up.
The Reality Check: What the Data Says
This is where the “matter-of-fact” reality hits. I looked at a systematic review of over a dozen clinical trials [Source 1] and a landmark PubMed review [Source 2] to see if fish-oil supplements actually halt the sort of brain inflammation that develops into full-blown dementia.
Here is the honest breakdown.
If you have, or your loved one has, already gotten a diagnosis of Alzheimer’s Disease, then the supplements don’t seem to do much. The data shows no significant reversal of cognitive decline once the disease is established.
However — and this is a big “however” — some researchers have identified what they call a “window of opportunity.” The stronger evidence points to earlier intervention — pre-clinical stages, or mild cognitive impairment — not after diagnosis.
We’re talking about people with Mild Cognitive Impairment (“MCI”) or people who are cognitively healthy but have a genetic risk, like the APOE4 gene — a genetic variant linked to higher Alzheimer’s risk — which we have gotten into in a previous video.
So, if you’re waiting for memory loss to start before you take your brain health seriously, you’ve likely missed the boat for Omega-3s to be effective.
If it’s anything, it’s better thought of as a preventative tool, not a rescue medication.
And even in studies that do show benefits, the effects tend to be modest — not dramatic.
The Metric: “Test, Don’t Guess”
One of the biggest reasons people see mixed results is that they aren’t actually measuring if the supplement is working. A paper in the journal American Journal of Clinical Nutrition [Source 4] argues that we should be focusing on something called the Omega-3 Index.
Most people just take a pill and hope for the best. But everyone absorbs fats differently. The Omega-3 Index is a blood test. It measures how much EPA and DHA are actually built into your red blood cells — which reflects long-term intake.
An index of ~8% or higher is the established cardiovascular target; brain health research is pointing in the same direction, though that threshold isn’t yet definitive.
If you’re taking a low-quality supplement or your body isn’t absorbing it well, you might still be at a 4% or 5% index — which is basically a deficiency zone.
If you aren’t testing your levels, you’re essentially flying blind. You might be taking a dose that’s too low to matter, or wasting money on a supplement your body isn’t even processing.
You can’t improve what you don’t track.
The Potential Problem: Oxidation and AFib
Now, we should address the “red flag” that’s been popping up in recent headlines.
A report from SciTechDaily [Source 5] highlighted a potential risk that many supplement companies don’t want to talk about: Oxidation.
Fish oil can be unstable. There’s concern that poorly stored or low-quality fish oil may oxidize or, to put it more dramatically, the worry is that it could go rancid when exposed to heat, light, or air.
Plainly, if it turned out that you were swallowing oxidized fish oil, then you wouldn’t be reducing inflammation — you’d potentially be introducing oxidative stress into your system.
But there’s a more specific medical concern. Recent data has linked high-dose fish oil supplementation to an increased risk of Atrial Fibrillation, or AFib — which is an irregular heart rhythm that can lead to strokes.
Now, I want to be careful with my language here, because this finding doesn’t quite fit the definition of an “outlier” that some have used to describe it. An outlier is a single anomalous data point. The AFib signal isn’t that — it has shown up across multiple large clinical trials, which actually makes it a replicated finding. That’s more serious, not less. The supplement industry might prefer you think of this as a fringe result. It isn’t.
This risk appears more pronounced at higher doses and in certain populations.
For example, in this case, the data suggests that “megadosing” fish oil — say, taking 4 or 5 grams a day without a doctor’s supervision — might be creating cardiovascular risks that outweigh the potential brain benefits, especially if you aren’t actually deficient to begin with. Which — again — you won’t know until your levels are measured.
And, to be fully transparent, some risk signals have appeared at lower doses too, particularly in prescription-grade formulations.
The honest bottom line is that the dose threshold isn’t perfectly established yet. Which is all the more reason to loop in your doctor before you dramatically increase your intake.
So yes — there’s a real risk conversation to have here, particularly around dose. But risk in context isn’t the same as “don’t bother.” It just means: be deliberate.
Conclusion: The Pragmatic Approach
So where does that leave us?
Omega-3s clearly matter for brain structure — but supplements aren’t a magic solution.
If you’re thinking about using them, a more grounded approach looks like this:
First: prioritize food. Fatty fish like sardines, mackerel, and salmon provide Omega-3s in a more stable, nutrient-rich form.
Second: if you do supplement, be picky. Fish oil is fragile — and quality matters. Choose third-party tested products. Look for labels like the dedicated, so-called “International Fish Oil Standards” program, or “IFOS” (/EYE-fohs/). And… If it smells off, don’t use it.
And third: know your numbers. The Omega-3 Index can tell you whether you’re actually in an meaningful range — or just guessing.
Because in the end, brain health isn’t about one supplement. It’s about maintaining the integrity of your brain over decades.
Fish oil may be one tool — but it’s not the whole toolbox.
If you found this helpful, consider subscribing for future breakdowns like this. And feel free to share it with someone who might benefit.
And, as always, we wish you all the best with your Alzheimer’s-proofing journey. Thanks for watching.
Sources:
[1]: https://pubmed.ncbi.nlm.nih.gov/28986068/ “Effectiveness of omega-3 fatty acid supplementation in patients with Alzheimer disease: A systematic review and meta-analysis – PubMed”
[2]: https://pubmed.ncbi.nlm.nih.gov/19523795/ “Omega-3 fatty acids and dementia – PubMed”
[3]: https://pubmed.ncbi.nlm.nih.gov/30084334/ “A Recent Update on the Effects of Omega-3 Fatty Acids in Alzheimer’s Disease – PubMed”
[4]: https://pmc.ncbi.nlm.nih.gov/articles/PMC9761771/ “The omega-3 index in Alzheimer’s disease: Ready for prime time? – PMC”
Given the research we do for this channel, I am no stranger to surprising, sometimes controversial—and occasionally disgusting—claims regarding Alzheimer’s disease.
In a previous video, we explored how something as mundane as earwax buildup—or, more technically, cerumen impaction—could lead to hearing loss and, by extension, cognitive decline.
Today, we’re looking at a physical habit.
It’s often dismissed as a minor social faux pas—and was even the subject of jokes in an old Seinfeld episode. But recent research suggests this common behavior might create a pathway for certain pathogens to reach the brain.
We’re talking about nose-picking—and its potential link to late-onset dementia.
For the companion video, see here:
The Griffith University Study
A team of researchers at Griffith University in Australia published a 2022 study in the journal Scientific Reports. They focused on a bacterium called Chlamydia pneumoniae.
This common airborne bacterium—sometimes called the Taiwan Acute Respiratory Agent—is primarily known for causing bronchitis and pneumonia. However, it has also been detected in a significant number of human brains affected by late-onset dementia.
Using mouse models, the researchers tracked how this bacterium travels. What they found was striking: it can move along the olfactory nerve—from the nasal cavity directly into the brain.
In these models, infection reached the central nervous system within 24 to 72 hours. Once inside, it triggered amyloid-beta deposition—the same protein associated with Alzheimer’s plaques.
One interpretation is that amyloid-beta may function as part of the brain’s immune response to infection. However, if that infection becomes chronic or repeatedly facilitated—potentially through damage to the nasal lining—this process could contribute to neurodegeneration.
In short: this research suggests that certain behaviors might make it easier for pathogens to access the brain.
Connection: The Earwax Analogy
You may remember from our earwax discussion that conductive hearing loss involves a physical obstruction—something like earwax blocking sound transmission.
In a similar way, the nasal epithelium acts as both a physical and immunological barrier.
The Griffith University study found that when this barrier was damaged, infections in the mice became significantly more severe.
Think of the nasal lining as a security checkpoint: if it’s intact, most threats are stopped. If it’s compromised, things can slip through.
Just as we cautioned against inserting objects into the ear canal, scientists now warn that picking—or plucking nose hairs—can damage this delicate lining. That damage may give pathogens a clearer route to the brain.
Why This Matters
As geriatrician Maria Carney noted in our earwax discussion, “most people don’t even realize that they have an issue.”
That lack of awareness is a recurring theme in both Alzheimer’s prevention and detection.
While nose-picking is often associated with children, it remains common in adults. In fact, one study found that about 91% of people admit to it.
I’m curious how that compares with this audience—so I’ve put up an anonymous poll if you’d like to weigh in.
As many viewers know, age alone—especially over 65—significantly increases Alzheimer’s risk.
If we add environmental exposures, such as introducing pathogens through repeated nasal damage, this could represent an additional, potentially modifiable risk factor.
Caveats and Disclaimers
To be clear: this is early-stage research conducted in mice. We do not yet have direct evidence that this pathway operates the same way in humans.
Human trials would be needed to confirm whether a similar mechanism is at work.
And of course, Alzheimer’s disease likely involves multiple contributing factors—including acetylcholine loss, plaque formation through other mechanisms, neurofibrillary tangles, and nutritional or metabolic influences.
So yes—this hypothesis may sound farfetched.
But it is being seriously explored, and it may be worth paying attention to.
Practical Advice and Conclusion
One of the core goals of the Alzheimer’s Proof project is prevention. And unfortunately, there is no single solution—no magic bullet.
What we can do is try to stack the odds in our favor.
Protect the Barrier
Avoid plucking nose hairs and minimize behaviors that could damage the nasal lining. Chronic irritation may increase vulnerability.
Use Safer Alternatives
If needed, consider electric trimmers for grooming. For congestion, saline sprays or nasal irrigation may help. If using a neti pot, always use distilled or properly purified water.
Keep It Clean
If you must manually clear your nose, ensure your hands are clean—before and after. Also keep fingernails trimmed and smooth to reduce the risk of micro-injury.
Stay Aware
Consult a healthcare provider if you experience persistent irritation, bleeding, or signs of infection.
The key takeaway here isn’t panic—it’s awareness.
Small habits, repeated over time, can shape long-term brain health.
And if reducing Alzheimer’s risk comes down—even in part—to eliminating preventable factors, then even small changes may be worth considering.
Anu Chacko, Ali Delbaz, Heidi Walkden, Souptik Basu, Charles W. Armitage, Tanja Eindorf, Logan K. Trim, Edith Miller, Nicholas P. West, James A. St John, Kenneth W. Beagley, and Jenny A. K. Ekberg, “Chlamydia pneumoniae can infect the central nervous system via the olfactory and trigeminal nerves and contributes to Alzheimer’s disease risk,” Scientific Reports, vol. 12, no. 2759, February 17, 2022, <https://www.nature.com/articles/s41598-022-06749-9>.
For decades, Alzheimer’s research has chased the same target — plaques and tangles.
And despite billions of dollars… results have been limited and often disappointing.
But… what if we’ve been aiming at the wrong problem entirely?
A new study suggests the real driver may be something more fundamental: inflammation.
And a compound called CBD might be able to dial it down.
Context: ‘Autoinflammatory’ Theory
To understand this breakthrough, we have to look at the “autoinflammatory” view of Alzheimer’s.
Traditionally, inflammation has been looked at as if it were a symptom of Alzheimer’s. But… researchers at Augusta University are arguing that chronic neuroinflammation is actually a core driver of the disease (along with other factors).
Translating that into dicey but everyday language, they’re starting to come around to the idea that inflammation is more of a contributing cause, not an effect.
Recall that, in general, “inflammation” is one of the body’s responses to illness or injury. In parts of our bodies we can see – an elbow, for instance (or…almost see!) – inflammation is what causes the hurt area to feel hot and painful, look red, swell in size, and so on.
Inflammation is often associated with loss of function. If your elbow is injured or inflamed, you can’t expect to be playing racquetball anytime soon.
Well… In Alzheimer’s disease, inflammation has to do with the brain’s immune system becoming chronically overactive. The brain gets stuck in a state of chronic immune activation. Yes, your brain can get inflamed, too.
This can also start a chemical chain reaction where usually functional neuronal “signals” begin to cause damage to nerve cells, instead of protecting them.
As a technical point, though, we don’t want to confuse inflammation (in the sense of haywire immune signaling and cellular activation) with what doctors call edema (i.e., large-scale fluid accumulation that increases pressure within the skull).
Think of it like this.
Your brain has a specialized immune system.
When it senses trouble, it sends out “first responders” like microglia and astrocytes.
In a healthy brain, these get to the scene of the accident, bandage the wounded, clean up, and go home.
But in Alzheimer’s, these cells get stuck in the “on” position. The emergency situation just goes on and on.
They stay “agitated,” and end up releasing toxic chemicals that (accidentally) kill the very neurons they were summoned to protect.
And this is where CBD enters the picture.
Science: IDO and cGAS
The study in question was led by Dr. Babak Baban. He and his team set out to see if cannabidiol, abbreviated “CBD,” could (so to speak) step into this mess as a peacekeeper.
CBD is already well known for its anti-inflammatory properties.
The researchers used a mouse model specially designed to mimic Alzheimer’s in humans.
They had these mice inhale CBD daily for four weeks. What they found wasn’t just “general” improvement. They identified two specific molecular “switches” that CBD was able to flip.
Two Molecular Switches
The first is an enzyme called IDO. It’s involved in how the brain processes tryptophan. You know, the essential amino acid that’s found in poultry – like your Thanksgiving turkey – which, by the way, has a largely undeserved “bad rep” for supposedly causing the “turkey coma” after you indulge. But that’s another story.
When overactive, IDO can shift tryptophan metabolism toward compounds that promote inflammation and neurotoxicity.
The second switch is a sensor called cGAS. This is basically a DNA-sensing pathway that can trigger powerful innate immune responses when activated.
In the Alzheimer’s-affected brains, both of these pathways were screaming at full volume.
But after the CBD treatment, the expression of IDO and cGAS dropped significantly.
Specifically, it quiets down the brain inflammation including in regions like the entorhinal cortex — a region critical for memory formation, and one of the first areas affected in Alzheimer’s.
By calming these two pathways, the CBD essentially told the brain’s immune system to “stand down.”
Results: Memory and Behavior
So, the biology changed, but did the behavior change? The symptoms?
Those are the “big” questions.
And the answer was… yes.
Remember, this is so far only demonstrated in animal studies. But…
The mice treated with CBD performed significantly better on recognition memory tests. And they showed more “exploratory behavior” than the untreated group. They weren’t just neurologically “calmer”; which researchers interpreted as improved cognitive function.
But here’s why this study is particularly exciting for the future of human medicine.
CBD appears to be a “multi-target” intervention.
While this specific study focused on inflammation, Dr. Baban’s team noted that their earlier work showed CBD may also influence plaque and tangle pathology through different mechanisms.
This is to say that, instead of a drug that only does one thing, we’re looking at a compound that might clear the trash, quiet the alarms, and protect the neurons all at the same time.
And notably, it’s derived from a plant.
Conclusion: The Road Ahead
Now. We have to be realistic.
This was only one study.
On mice.
While mouse models are essential for understanding these brain “switches” in a generic sense, humans — and our brains — are much more complex.
We still need rigorous human clinical trials to see if these results translate, what the right dosage is, and if long-term use is safe for seniors.
But…
If this line of research holds up, it changes the entire strategy.
Not just clearing damage — but preventing it at the source.
Not a single target — but an entire system reset.
And that raises a bigger question: Have we been looking for a silver bullet… when Alzheimer’s is really a systems-level failure?
If so, the future of treatment may not look like a drug that does one thing — but a therapy that brings the brain back into balance.
The question is: are we ready to rethink everything?
Including that an answer to one of our most complex diseases might be found in the chemistry of one of our most misunderstood plants.
What are your thoughts? Do you think the future of Alzheimer’s treatment lies in CBD, or are you still skeptical of cannabis-based medicine? Or are you more skeptical of pharmaceutical treatments? I’d love to read your comments.
By the way, if you’re interested in this idea of multi-target therapies, we’ve explored it before. In one video, we break down how CBD and THC interact with the brain.
And in another, we look at the controversial research into Lysergic acid diethylamide (or “LSD” and dementia — where, interestingly, a similar “systems-level” approach has been proposed. So if this direction intrigues you, those are worth watching next.
AT A GLANCE: Amyloid‑β plaques = a hallmark of Alzheimer’s disease; Most drugs target plaques directly
Alzheimer’s may involve a failure of brain “cleanup,” not just toxic buildup.
What if Alzheimer’s isn’t just caused by toxic buildup in the brain — but by the brain’s own cleanup crews being quietly dismantled from the inside?
If you’ve been around the block, when it comes to Alzheimer’s, you probably realize that a primary “pathological hallmark” is the accumulation of – what are called – “amyloid-beta plaques” within the brain.
AT A GLANCE: What if the problem is impaired clearance—not just plaque formation?
For over a century — since Alzheimer’s was first described in 1906 — drug development has largely focused on stopping plaque formation or clearing plaques after they appear.
And a critical area of this investigation involves taking a close look at the brain’s innate ability to clear these toxic proteins.
Recent research from the Indiana University School of Medicine has identified a specific enzyme that, when it is present, appears to be a factor when someone’s brain-clearing mechanisms go haywire.
And, in this video, we’ll look at a CliffsNotes’ version of the results.
AT A GLANCE: IDOL = Inducible Degrader of the LDL receptor controls how many LDL receptors remain on brain cells
The enzyme is abbreviated I‑D‑O‑L, or “IDOL,” short for “Inducible Degrader of the LDL receptor.” That expression (a mouthful, for sure) designates a protein that controls how many LDL receptors survive on the surface of brain cells.
But… what the heck is it? And, more importantly, how would its inhibition (quote, unquote) represent a promising shift in doctors might approach Alzheimer’s treatments?
The Molecular Rôle of “IDOL”
AT A GLANCE: Receptors = cellular “locks” that trigger actions
To even begin to understand this discovery — and to be perfectly honest, that’s about the most ambitious goal I can realistically aim for — we need to talk about something called a low‑density lipoprotein, or “LDL,” receptor.
First, in the relevant context, a “receptor” is a protein on a cell — or in a cell — that acts like a lock. When the right chemical “key” comes along, that lock opens and tells the cell to do… something.
AT A GLANCE: LDL receptors pull material into cells for use or disposal
An LDL receptor is one of these locks. Its job is to grab so‑called “bad” cholesterol — LDL — and pull it into cells so it can be used or gotten-rid-of.
Think of it like a trash‑pickup claw that grabs garbage from the streets of the body and pulls it inside for disposal.
AT A GLANCE: In the brain, LDL receptors help manage APOE and amyloid‑β
In the central nervous system, LDL receptors also play a crucial role in regulating APOE, a protein involved in the transport and clearance of amyloid‑beta.
So far, so good?
AT A GLANCE: IDOL tags LDL receptors for destruction
Now for this IDOL business.
IDOL is not a receptor itself. It’s a protein that comes along and “tags” LDL receptors for destruction — that’s the “inducible degrader” part of its full name.
AT A GLANCE: Overactive IDOL à fewer LDL receptors; (-) Amyloid clearance à (+) plaque buildup
It’s like removing the trash‑pickup claws and throwing them away instead of the “bad” cholesterol. Reducing the number of LDL receptors on cell surfaces is a bit like getting rid of trash trucks in the heart of a crowded city. It’s not good.
When IDOL becomes overactive, too many LDL receptors are destroyed, weakening the brain’s ability to clear APOE and toxic amyloid‑beta proteins. This allows plaques to accumulate and neurodegeneration to accelerate.
In effect, an overactive cellular “shutdown switch” disables the brain’s cleanup crews at precisely the moment they’re needed most.
Receptor Inhibitors — and Why IDOL Is Different
AT A GLANCE: IDOL inhibitors protect receptors; They stop destruction — not signaling
At this point, it helps to understand what scientists mean by a “receptor inhibitor.” Usually, a receptor inhibitor blocks a lock so that even when the correct key shows up, the cell can’t respond. But that’s not quite what’s happening here.
An IDOL inhibitor doesn’t block the lock — it stops the demolition crew from tearing the lock off the door. In other words, inhibiting IDOL prevents LDL receptors from being destroyed, allowing the brain’s cleanup machinery to stay in place and keep doing its job.
IDOL Proteins Aren’t the Problem in and of Themselves
Let’s register a couple caveats.
Number one, it’s important to understand that IDOL proteins aren’t “bad” in and of themselves. They’re normal control mechanisms within the complex anatomy-biology of the body.
And they don’t come from “outside.” Your own cells make IDOL proteins automatically.
AT A GLANCE: IDOL is a normal control mechanism; Problems arise when it shuts things down too aggressively
Think of their part in in the trash-removal process as akin to that of a “thermostat” that off the air conditioner or furnace when the desired temperature is reached. When a cell thinks it’s cleaned up enough LDL cholesterol, these IDOL proteins shut down the whole process.
In the context of Alzheimer’s Disease, overactive IDOL proteins lead to a depletion of these trash-removal receptors. In turn, this loss diminishes the brain’s capacity to clear amyloid-beta. And that, researchers, suspect, leads to – or makes worse – the formation of the plaques that lead to neurodegeneration.
Whew!
AT A GLANCE: Evidence so far: animal + cellular studies
It’s also important to note that this entire IDOL–LDL receptor mechanism has been demonstrated primarily in animal and cellular studies. While the evidence strongly implicates IDOL in Alzheimer’s pathology, human treatments are still in-process.
Research Findings
Neuronal vs. Microglial IDOL
AT A GLANCE: Microglial IDOL removal à little effect; Neuronal IDOL removal à major plaque reduction]
The study in question was led by Dr. Hande Karahan and Dr. Jungsu Kim, who sought to determine which cell types were most responsible for IDOL-mediated damage. Historically, the scientific community focused on microglia — the brain’s immune cells — as the primary drivers of plaque-clearance.
However, using a series of “knockout models,” the Indiana University team found that removing IDOL from microglia had a negligible effect on plaque levels.
AT A GLANCE: “Knockout” = a gene deliberately switched off to study its function
A “knockout model” is a genetically engineered animal — usually a mouse — in which a gene like IDOL is “switched off” so scientists can see how the brain behaves without it.
They take out a gene to see what breaks — or improves — when it’s gone.
When IDOL was “deleted” specifically from neurons, the results were deemed significant. The researchers observed a substantial reduction in amyloid-beta deposition.
AT A GLANCE: Lower APOE4 levels observed; APOE4 = strongest genetic risk factor for late‑onset Alzheimer’s
Additionally, the deletion of neuronal IDOL led to a decrease in APOE4 levels. As APOE4 is the most significant genetic risk factor for late-onset Alzheimer’s, this suggests that targeting IDOL could directly mitigate the risks associated with this specific genotype.
Clinical Implications and Synaptic Health
AT A GLANCE: IDOL inhibition linked to improved ‘synaptic plasticity’; Healthier connections = better learning & memory support
What distinguishes this research from current treatments — such as antibodies that target existing plaques — is its focus on enhancing the brain’s internal environment.
The researchers also observed a second effect – beyond reducing toxic amyloid-beta. This is to say that inhibiting IDOL was also associated with improvements in synaptic plasticity — the brain’s ability to adjust and strengthen connections involved in learning and memory.
It refers to how the brain “rewires” itself.
Conclusion: The Path to Small-Molecule Therapeutics
AT A GLANCE: Targeting IDOL may improve the brain’s internal environment
From a pharmaceutical perspective, the IDOL enzyme is a highly viable (read: commercially promising) target.
So, the upshot is that drug-researchers believe they may be able to engineer an oral medication capable of inhibiting the trash-removal inhibition!
AT A GLANCE: Goal: oral drugs that cross the blood‑brain barrier; Less invasive than antibody infusions
From a cost-per-treatment standpoint, this would an advancement over the current method, which requires expensive – and invasive – intravenous infusions required to deliver antibody treatments to try to dissolve plaques.
The Indiana University School of Medicine team is still a “preclinical” phase. Its focus is on screening for “small molecules” that can effectively cross the blood-brain barrier to inhibit IDOL. While further trials are obviously necessary, this research provides a roadmap for a new generation of Alzheimer’s therapies.
For those you still here, thank you for sticking with it! I know it was heavy-going.
If you’d like to dig deeper, here’s a link to the original study — because this is one of those cases where the data itself really is the story.
What if a simple sleeping pill could help the brain wash away the very proteins linked to Alzheimer’s disease? A surprising new study suggests that an already FDA-approved insomnia medication may do exactly that.
Researchers have found that a common, Food-and-Drug-Administration-approved sleeping pill might actually reduce the buildup of toxic proteins linked to Alzheimer’s disease.
Today, we’re diving into the reportage of the science behind this discovery. And we’ll discuss a bit about what it could mean for the future of dementia prevention.
The Study
First thing’s first: The study we’re concerned with was written up in an article titled “Suvorexant Acutely Decreases Tau Phosphorylation and Aβ in the Human CNS,” which was published online in the March, 2023 edition of the scientific journal Annals of Neurology. And it was printed in a hard-copy version in July of the same year.
To understand the study, we first need to understand how the brain ‘cleans’ itself (quote, unquote) during sleep.
While we sleep, our brain uses something called the “glymphatic system.” Think of it like a biological dishwasher. It flushes out metabolic waste that builds up while we’re awake.
Two of the most dangerous types of “trash” cleared out by this glymphatic system are amyloid-beta and tau proteins.
Of course, viewers of this channel — not to mention anyone with a basic familiarity of Alzheimer’s — probably won’t fail to recognize these words.
After all, it’s these proteins that, when not cleared effectively, clump together into the notorious “plaques and tangles” that constitute the hallmarks of Alzheimer’s disease.
This is one reason why chronic sleep deprivation is often cited as a major risk factor — alongside advanced age, of course — for cognitive decline.
Suvorexant
Enter a drug called suvorexant, known by the brand name “Belsomra.”
It’s a type of drug known as an “orexin-receptor antagonist.” Oversimplifying, orexin is a molecule in the brain that keeps us awake and alert.
The idea is that, by blocking orexin, the drug suvorexant may encourage the brain to transition into sleep.
Researchers at Washington University School of Medicine in St. Louis, Missouri wanted to see if using this specific drug to “promote” or “enhance” sleep could help to lower the levels of the aforementioned toxic proteins.
To this end, and as scientific studies typically do, they took a group of thirty-eight healthy volunteers, aged 45 to 65, and gave them either a dose of suvorexant or a placebo before bedtime. Researchers then monitored the participants’ cerebrospinal fluid over the next 36 hours.
What Happened?
To hear them tell it, the results were striking.
In the subset of participants who took the higher-than-usually-prescribed dose of suvorexant, levels of amyloid-beta dropped by 10 to 20 percent, compared to the placebo group.
Even more significantly, the same group saw a drop in “phosphorylated tau” — a form of the tau protein that is particularly closely linked to brain-cell death and Alzheimer’s- disease progression.
What makes this exciting is that it wasn’t just “better sleep” clearing the brain (in some vague sense); it was a specific intervention that seemed to target the very precursors of Alzheimer’s pathology.
Caveats
However, before we get too ahead of ourselves, there are some major caveats.
This was a very small study, and it only lasted for two nights. Therefore, researchers cannot yet say if taking this medication, long-term, will actually “prevent” dementia, or if the protein levels will stay low once the medication is stopped.
The researchers themselves prefer to refer to this as something more like a “proof-of-concept.”
Of course, we would want to see much longer trials to decide if the observed reduction in proteins actually translates into a predictable — and reliable — reduction in cognitive decline.
That said, this study confirms that the intersection of sleep medicine and neurology is one of the most promising frontiers in medicine. And it suggests that we might eventually treat sleep not just as a lifestyle habit, but as a clinically significant tool that may help us to maintain brain health as we age.If you’re interested in the full details of the study, click for the ScienceAlert article or for the original paper. We hope you rest a little easier tonight!
When I was a kid, and I heard “adults” saying: “Oh, they grow up so fast,” I probably rolled my eyes. I mean, how obvious can you get, right?!
Now I have two sons – both in their early 20s. Now I know what “they grow up so fast” means.
Similarly, I didn’t need my dad and grandma to get Alzheimer’s Disease to know that “dementia is bad.”
But it’s a bit like “they grow up so fast.” Sometimes, the things you’ll nod your head (in agreement) to, don’t really sink in until you’ve had a certain amount or type of experience.
So, here’s what I’ll do in this video. I’d like to list five (5) things that probably seem so obvious that I don’t think I ever would have denied them.
At the same time, from where I sit now, I realize that I didn’t actually appreciate the full significance of any of the five until I became the daily caregiver for my dad around 2008.
(The video version of this presentation is available on our YouTube channel.)
My dad died in 2016 from complications related to his Alzheimer’s. I have had several years to decompress and reflect on my family’s experiences with that dreaded disease.
So, I don’t say that just being my dad’s caretaker illuminated my mind. And I won’t pretend that merely listing these things for you will illuminate yours.
At the same time, I feel like encouraging you to slow down and maybe meditate on these things might be worthwhile. So, okay…
Dementia can change your loved one’s entire personality.
If, pre-2008, you’d have asked me: “Can Alzheimer’s alter personality?” I’m sure I’d have said, “You bet.” Nevertheless… Here’s what I thought when I started caretaking.
I thought my dad would continue to be the same extroverted, happy-go-lucky, laid-back person I had always believed him to be. – just with increasing memory problems. It took months – and countless frustrating, tearful, and sometimes (frankly) scary interactions – to learn that Alzheimer’s had flipped his personality. Almost all my dad’s traits that I just listed literally turned into their opposites. He was withdrawn and isolated, combative, agitated, etc.
Now… a case can be made that all these “negatives” had always been there, deep down. Everyone has a “dark side,” kind of thing.
So, maybe, for most of his life he was just really good at hiding or restraining those parts. And, maybe, when he got Alzheimer’s, he just couldn’t or wouldn’t hold back any more. Regardless…
What you “get” – when caring for a dementia-afflicted loved one – is often quite different from what you’re used to, what you expect, and especially what you hope for. So, be prepared for anything! Or, to put it another way, realize that the person you’re dealing with – while they may resemble the one you’ve known and loved your entire life – might act like a complete stranger.
Being a caretaker can make you feel really depressed.
Again, is this a surprise? Even people with no experience with Alzheimer’s probably know that it’s a horrible – and terminal – disease. Watching a loved one deteriorate is depressing.
But I thought that I’d at least feel as if I were doing something worthwhile by helping my dad.
And, don’t get me wrong, it was worthwhile, objectively speaking. In hindsight, I do cherish the fact that I was present for and with my dad.
Subjectively, though, when everything was going on, I felt miserable. Caretaking frequently felt futile and useless. And I felt physically sick much of the time. Maybe it’s just me.
It wasn’t just the understandable fact that my dad didn’t appreciate what I was doing. It was that he resented and actively resisted me. The whole thing was a fight practically from day one.
I locked the doors from the inside. I hid his tools. I disabled the car and – ultimately – pushed his long-time doctor to petition the state to get his driver’s license revoked. I was the enemy.
I knew that the steps I took had to be taken. But it was also painfully obvious my dad was being systematically cut off from all the things that gave him freedom and that he always loved to do.
I tried to remind myself that his disease was really to blame – not me. But that didn’t stop me from being overcome with guilt and regret. I’ve gotten more into all this in a dedicated video.
So: If being a caregiver makes you feel awful, you’re not alone. I felt horrible.
And, on the wavelength of things I didn’t fully know: Know that your life – and the life of your loved one – may be permanently changed. Relatedly…
You will need to take breaks.
Not taking a break can lead to serious consequences – not least is your own emotional or physical breakdown and burnout. Who would deny it?
By the same token, you can’t exactly leave an Alzheimer’s sufferer by themselves for any length of time. It may be difficult for you to prepare and eat meals in peace or to get an uninterrupted night’s sleep, let alone to take a mini-vacation. And this can go on for years.
In our case, my dad would live nearly eight (8) years after his diagnosis. That’s a long time to be someone’s 24/7 caretaker all by yourself.
So… how are you going to take those needed breaks?
As I’ve mentioned in other presentations, if you have no able or willing family members to relieve you from time to time, or in an emergency, then you may have to turn to professionals. Adult daycare, home-care providers, and (what are called) respite-care specialists can all play rôles, here. But, however you get help, you need to make sure that you take care of yourself.
Ultimately, a nursing home or other long-term care facility may be the only game in town. And on that note, try to more fully appreciate that…
Your loved one may end up in a nursing home.
And when I say “end up,” I don’t mean to suggest that it’s inevitable. I don’t believe that.
And, in my case, I don’t mean to refuse responsibility for the decision to get him admitted. It was my choice.
But, honestly, early on, I did a lot of “ostriching.” If I had seriously faced the fact that a nursing home was a possible – or eventual – outcome, I’d like to think that I would’ve planned for it.
I’d say: “I would have planned better.” Except, to be frank, I didn’t do any real planning at all.
No one in my family wanted to think about dad being in a nursing home. – including me.
And I put off any serious thought about that option until I was totally exhausted with caretaking. By that time, our options were severely limited. Even among homes we could “afford” (quote, unquote), our top two (2) choices were unavailable. They both had year-long waiting lists.
And because I was emotionally broken when I started to look into various homes, it’s likely that I didn’t investigate as thoroughly as I might have. – or, quite possibly, as I should have.
Since you can’t reason well when you’re under duress, my evaluation of the options – and my decision – were probably compromised also. It would have been healthier for me to admit, from the get go, that I couldn’t really rule out nursing homes.
If I’d have done only that, our decision-making process would have gone much better – and, possibly, yielded a better outcome. To top it off, I didn’t fully appreciate that…
A nursing home isn’t a perfect solution.
Again, who would say otherwise? For one thing, it’s obvious – at a general level – that when we’re deciding between two or more options, each choice will have positives and negatives.
Duh. Right? In hindsight, it seems pitifully naïve of me to have ever hoped that a nursing home would be “the answer to all my prayers.” Of course, nursing homes have their own drawbacks.
Some of these disadvantages are both major and pretty obvious – like the fact that they have a staggering, current average cost in the vicinity of $8,000 per month.
Another serious downside – one that I intend to make the focus of its own video – is the arguable tendency of nursing homes to over-medicate their patient-residents. I don’t want to go too far down this rabbit trail right now. Let’s just say that – in my opinion – my dad’s nursing home medicated him just to make him docile.
But it was hard for me to understand all this when I was at the end of my rope with homecare. The situation became seriously unmanageable. And I became desperate for an escape route.
So, at the risk of concluding with another one of those aphorisms that’s easy to say, but hard to appreciate or do… Try to stay as clear-headed as possible.
From a practical standpoint, try to have open and honest conversations with every interested person in your circle: from family and friends to doctors, lawyers, and so on.
Solicit advice from as many reputable sources as possible. And run your options past your family “think tank.” Try not to exclude any possibilities.
In two (2), planned, follow-up videos, I’ll expand on some of these ideas and explore related topics like “things I wish I’d known when I started off caretaking.” In the very next installment, already written, I’ll suggest three (3) things that I would do immediately, if I had to be a caregiver all over again.
But if you found something of interest or of use in this video, I invite you to click “Like.” It helps YouTube know that you appreciated the presentation.
If you’d be interested in hearing some of my tips, then please Subscribe to the channel (if you haven’t already) and don’t forget to make sure your notifications are turned on – the “bell” icon.
And if you think someone else might get something out of the video, kindly share the original link on your social media pages.
Either way, though, I thank you for watching.
And I wish you all the best for your caretaking efforts.
In February of 2023, the family of actor Bruce Willis revealed that he has a form of cognitive impairment called “frontotemporal dementia.” While not the same condition as Alzheimer’s Disease, proper, the sad announcement provoked a flurry of increased traffic to the Alzheimer’s Association’s website. In other words, the disclosures started a renewed conversation about aging – and its attendant illnesses.
For me, this is not simply an academic matter. My dad, Jim, died from Alzheimer’s Disease in 2016 after a decade-long struggle with that dreaded condition.
Going through the experiences of trying to care for him and, later, getting him situated in – and visiting – a nursing home, I often felt that we were alone. Of course, and unfortunately, that is far from the case.
But, frequently, it’s not exactly public knowledge that a person has Alzheimer’s (or some other form of dementia).
One reason is the (pretty straightforward) consideration that families of all sorts usually wish to maintain their privacy in such matters.
Another is that Alzheimer’s is an insidious ailment whose presence may not be obvious until it is fairly advanced.
Finally, we don’t all have celebrity status! But, for those who – enviably or not – have achieved some measure of fame, it may be a different matter.
So, in this video, I will run through some of the “stars” of the stage or screen who are known to have had the misfortune of an Alzheimer’s diagnosis – and the ensuing cognitive decline and debilitation.
Caveats
I do not mean for this to be lurid or sensational. On the contrary, one chief purpose is to remind viewers that dementia is no respecter of persons, as it were. As far as we know, and notwithstanding various hypothesized predispositions and risk factors, Alzheimer’s Disease can strike almost anyone. So, for those who are dealing with this terrible affliction, let this serve as a tragic reminder that you’re not alone.
A further purpose is more practical. I’m trying to get back into the swing of making videos for this channel! And, yes, I have plenty more practical content planned. So…stay tuned!
The Top Ten
10. Joanne Woodward
At 93 as of this writing, Joanne Woodward is the only entrant on this list to be alive at time of recording.
Getting her start in television in the early 1950s, she broke into a major movie rôle in the 1956 crime drama A Kiss Before Dying, with Robert Wagner.
Indisputably, her breakout performance came the following year in the psychological drama The Three Faces of Eve, for which she won the Academy Award for Best Actress in 1958.
She would be nominated for further recognition for the 1968 drama Rachel Rachel, directed by her longtime collaborator and late husband, Paul Newman.
Her critical acclaim extended into the 1970s, where she performed in Gilbert Cate’s 1973 Summer Wishes, Winter Dreams.
As the decade progressed, she transitioned back into t.v., where – among other accolades – she won an Emmy Award for the 1978 production See How She Runs.
Sadly, in an article that appeared in the Los Angeles Times in 2022, we read: “Diagnosed with Alzheimer’s disease in 2007, Woodward has retreated from public life.”
9. Robert Loggia
Born Salvatore Loggia on January 3, 1930, he studied journalism in college. But the man who would become known as Robert Loggia rose to fame primarily playing “tough-guy” rôles. For example, he played the lead in Walt Disney Presents 1958 television series “The Nine Lives of Elfego Baca.”
Loggia’s face seemed ever-present especially during the 1980s, where he made notable appearances in several widely distributed films, including 1982’s An Officer and a Gentleman with Richard Gere.
The following year, he starred alongside Anthony Perkins in Universal Picture’s sequel to Alfred Hitchcock’s groundbreaking 1960 horror film, Psycho.
But frequently, Loggia was cast to play mobster-type characters. For example, he was a Miami-based cocaine smuggler and “drug lord” in Brian de Palma’s 1983 Scarface, which also featured Al Pacino.
Or, again, he was cast as sleazebag smut producer “Mr. Eddy” (also called “Dick Laurent”) in David Lynch’s 1997 abstract, psychological thriller, Lost Highway.
Occasionally, these secondary parts garnered him critical acclaim. For instance, Loggia was nominated for an Academy Award for Best Supporting Actor for his portrayal of private investigator Sam Ransom in the 1985 crime mystery, Jagged Edge.
And he won a Saturn Award in 1990 for his rôle as a toy-company owner in the 1988 “dramedy” Big, starring Tom Hanks.
Robert Loggia was diagnosed with Alzheimer’s disease in 2010. He passed away from its complications on December 4, 2015, at the age of 85, at his home in Brentwood, Los Angeles.
8. Burgess Meredith
Born in Cleveland, Ohio in 1907 (November 16), Oliver Burgess Meredith began his acting career in the 1930s on Broadway.
His early cinematic work includes, with Lon Chaney Jr., a 1939 adaptation of John Steinbeck’s Of Mice and Men and, …
…with Robert Mitchum, a starring rôle in 1945’s The Story of G. I. Joe.
Meredith was lauded for his acting in John Schlesinger’s 1975 historical satire, The Day of the Locust.
He was also well known to popular audiences for his work on television. During the 1960s, Meredith made a handful of appearances on Rod Serling’s The Twilight Zone, …
…and, as the villain the “Penguin,” on Batman, alongside Adam West and Burt Ward.
During the late 1970s and early 1980s, Meredith was a fixture in Sylvester Stalone’s blockbuster Rocky franchise, where he portrayed the gravelly voiced trainer, Mickey Goldmill.
After over fifty years of memorably quirky performances, in 1997, Meredith passed away. CNN reported his death, noting that Meredith “had been suffering from melanoma and Alzheimer’s disease”. He was 89.
7. Eddie Albert
The man who would attain celebrity under the name “Eddie Albert” was born Edward Albert Heimberger in Illinois in 1906.
He was successful both on television and on the “big screen.” Though, for a while, it seemed that his career would end prematurely. At one time, and (incidentally) similarly to Burgess Meredith, Albert’s name was associated with Hollywood’s so-called “blacklist.”
This was primarily because of his wife Margo’s suspected left-leaning political sympathies and her alleged acquaintance with members of the Communist Party.
However, Albert’s stellar record during World War Two, helped salvage his career. He was regarded as a hero because, as a naval steersman, he rescued 47 marines that were pinned down with gunfire.
Albert subsequently appeared in William Wyler’s 1953 comedy, Roman Holiday, for which he received a nomination for the Academy Award for Best Supporting Actor.
For six seasons, between 1965 and 1971, he starred with Eva Gabor in the once-popular “sitcom” Green Acres. Albert played the character Oliver Wendell Douglas, a lawyer who gave up his practice to become a farmer.
He was again nominated for Best Supporting Actor for the 1972 comedy The Heartbreak Kid, which is now ranked #91 in the American Film Institute’s list of 100 all-time funniest movies.
During the 1980s, he was also featured on the prime-time CBS series Falcon Crest, a soap opera revolving around a prestigious vintner played by Jane Wyman.
When he died at home near California’s Pacific Palisades, it came out that Eddie Albert had been diagnosed with Alzheimer’s Disease around 1995.
Though, according to his son, he had continued to be active right up to his death. The official cause of death was said to be pneumonia. Albert was 99 years old.
6. Charles Bronson
Born Charles Dennis Buchinsky in Pennsylvania in 1921, he forged himself into “Charles Bronson,” a personality that – in many ways – exuded gritty toughness onscreen and off.
The name change, by the way, was suggested by his talent agent. The supplied reason will sound familiar by now. Specifically, “Buchinsky” was thought to be a little too Eastern-European-sounding for a nation currently conducting House Un-American Activities Committee proceedings trying to ferret out Communist infiltrators. Bronson appears to have come through the period unscathed.
Among the most successful action movies to his credit are the titular rôle in so-called “B-Movie King” Roger Corman’s 1958 Machine Gun Kelly,
John Sturges’s 1960 production, The Magnificent Seven, …
…and the same director’s 1963 film, The Great Escape, …both of which starred Steve McQueen.
…Robert Aldrich’s 1967 war picture, The Dirty Dozen, …
…and Sergio Leone’s 1968 “spaghetti western,” Once Upon a Time in the West, …
But, Bronson’s most recognizable character was as “Paul Kersey,” a once mild-mannered professional who turns to vigilantism when his wife is slain after a home burglary.
The original franchise – known as the Death Wish series – consisted of some five installments over twenty years.
It was remade in 2018 by Eli Roth, with Bronson’s rôle played by Bruce Willis, whom we mentioned in our introduction. This has added poignancy given that both actors have been associated with dementia.
In Bronson’s case, news outlets revealed in 2001 that he was “battling Alzheimer’s.”
Charles Bronson died August 30, 2003 at the age of 81.
Sidelight
Although I may devote a dedicated video to the topic, I’d like to acknowledge that numerous individuals have suffered from other forms of dementia besides Alzheimer’s Disease.
Of course, we have already registered this point in reference to Bruce Willis, who is said to suffer from Frontotemporal Dementia. But, there are a number of others who could be mentioned here as well. I’ll simply list three.
The first was actor George Sanders. A highlight of his career was winning the Academy Award for Best Supporting Actor in 1951 for his performance in Joseph L. Mankiewicz’s 1950 drama, All About Eve.
Sanders’ apparent suicide in 1972 was – perhaps – at least partially attributable to his dementia (which was, as far as I can tell, of an unspecified sort).
Or, again, we have actress Estelle Gettleman. Born Estelle Scher, she is better known by her stage name Estelle Getty. She had sporadic, odd rôles early in her life. But her main claim to fame came as the character Sophia Petrillo on NBC’s hit comedy series The Golden Girls, which ran from 1985 to 1992.
Getty died in 2008 from complications arising from Lewy-Body Dementia.
Finally, I’ll quickly mention comedy icon Robin Williams. Known for his wacky and improvisational style, his film and television credits are too numerous to relate exhaustively. But standouts include Aladdin (1992), Good Morning, Vietnam (1987), and Mrs. Doubtfire (1993).
Williams also “starred” in many noteworthy dramas – albeit, frequently with a touch of Williams’ characteristic humor – including Dead Poets Society (1989), Fisher King (1991), Good Will Hunting (1997), and What Dreams May Come (1998).
But, a darker side emerged in such movies as The Secret Agent (1997), based on Joseph Conrad’s 1907 novel, and Christopher Nolan’s Insomnia (2002).
Like Estelle Getty, Robin Williams may have had Lewy-Body Dementia – although, this fact was not disclosed until autopsy results were made public after Williams’ death.
And, of course – tragically – like George Sanders, Robin Williams was said to have taken his own life.
5. Peter Falk
Peter Michael Falk was born September 16, 1927 in New York City. His identifying squint was caused by the artificial eye he was forced to use after his natural eye had to be removed because of cancer when he was three years old.
Falk got his start in theater, but transitioned into the world of motion pictures. Among his credits are a disturbingly gritty portrayal of a mob-connected killer in the 1960 gangster film Murder Inc., …
…and Frank Capra’s 1961 comedy, A Pocketful of Miracles.
Much later, Falk appeared as both “grandpa” and narrator in Rob Reiner’s lighthearted 1987 The Princess Bride.
Still, there is little question but that Falk was most famous for his television work as the perceptive but self-effacing detective Columbo – which rôle he reprised over several broadcast seasons.
Following two successful “pilots” in 1968, the show ran from 1971 to 1978 and then continued from 1989 to the early 2000s. Falk is still instantly visually recognizable as Lieutenant Columbo. And he played the part with a humorous edge, as illustrated by his trademark line – “Just one more thing, …” – always delivered before the final mystery “reveal.”
In December of 2008, news outlets reported that the actor had been diagnosed with Alzheimer’s Disease.
At a “conservatorship” hearing the following year, a physician testified that Falk had “slipped rapidly into dementia since a series of dental operations in late 2007” – at least, according to a summary from the Huffington Post.
The article then went on to raise obliquely the possibility – underdetermined by the evidence at hand – that the Alzheimer’s had been brought on, or “worsened,” by the anesthesia.
In any event, he died at 83 on June 23, 2011.
A gossip page asserted that Peter Falk’s “official cause of death was cardiorespiratory arrest, while pneumonia and Alzheimer’s Disease were both ‘underlying causes’ …”.
4. Gene Wilder
Born Jerome Silberman in Milwaukee, Wisconsin on June 11, 1933, the boy who would eventually be known as “Gene Wilder” had humble beginnings. His father and maternal grandparents were Russian-Jewish immigrants.
Beginning his movie career in 1967 with Bonnie and Clyde, which featured Faye Dunaway and Warren Beatty in the titular roles, he moved onto a long-time and lucrative partnership with comedy director Mel Brooks.
Wilder performed in numerous films, including, in 1967, The Producers, as well as Blazing Saddles and Young Frankenstein, both in 1974.
He married Saturday Night Live actress Gilda Radna. When she died at 42 from ovarian cancer, Wilder promoted cancer awareness.
But his most memorable rôle – not least through its generation of at least once persistent “meme” [Note: This remark will be elucidated via an onscreen image. – M.B.] –…
… might be as a quirky chocolatier in the 1971 movie Willy Wonka and the Chocolate Factory.
Gene Wilder died at the age of 83 in his home in Connecticut on August 29, 2016.
The cause, not publicly disclosed until after his death, was Alzheimer’s Disease.
Posthumous statements from relatives stated that he had been diagnosed in 2013, but that the star chose to keep the news from fans so as not to distress anyone.
Poignantly, in one press report, Wilder’s nephew was quoted as saying that his uncle “…simply couldn’t bear the idea of one less smile in the world.”
3. Charlton Heston
“Charlton Heston” was the well-known stage name of the man born John Charles Carter.
As a movie star, he was especially recognizable for his portrayal of major religious figures in several prominent productions during the 1950s. For example, Heston was cast as the Biblical Moses in iconic director Cecil B. DeMille’s final – and most successful – films, The Ten Commandments, released in 1956. The part earned him a Golden Globe nomination.
Four years later, Heston won the Academy Award for Best Actor for his performance in William Wyler’s 1959 Christian-themed epic, Ben-Hur.
He is also remembered for several striking works of dystopian fiction, including the influential 1968 sci-fi movie Planet of the Apes, …
…and the 1973 horror “cult classic” Soylent Green.
Perhaps his most controversial rôles, however, were in the political sphere. Initially, his activism was in the service of left-leaning causes advanced by the Democratic Party. For instance, Heston spoke in favor of the Civil Rights Movement during the 1960s.
During the 1980s, he changed his allegiances and became a Republican. In this capacity, Heston served as a spokesman for, and president of (1998–2003), the gun-rights-advocacy group known as the National Rifle Association, for whom he popularized the slogan “I’ll give you my gun – when you pry it from my cold, dead hands.”
On August 9, 2002, it was widely reported that Heston had been diagnosed with “a neurological disorder whose symptoms are consistent with Alzheimer’s disease.”
Heston vowed that he was “neither giving up nor giving in”.
Roughly a year later, in what would prove to be his final public appearance, he was given the “Medal of Freedom” in 2003 by then-U.S. President, George W. Bush.
Despite this, his decline was rapid.
By 2005, Heston was apparently bed-ridden much of the time.
Ultimately, he passed away April 5, 2008 at the age of 84. The immediate cause was subsequently given as complications due to pneumonia.
2. Rita Hayworth
Rita Hayworth was born Margarita Carmen Cansio on October 17, 1918 in Brooklyn, New York.
In the 1940s, along with Betty Grable, Veronica Lake, Carole Landis, Marie McDonald, Jane Russell, and others, Hayworth became a popular “pin-up girl” for many U.S. soldiers.
Given this, it’s not a surprise that she was cast alongside Gene Kelly in the popular wartime musical Cover Girl (1944).
Hayworth got her “start” on the silver screen appearing in B-movies, such as the 1937 mystery, The Shadow.
But her first major dramatic role – and possibly her most enduring – was as the lead femme-fatale character in the 1946 movie Gilda.
Other of her numerous film credits include: Only Angels Have Wings (1939), The Lady from Shanghai (1947), and Pal Joey (1957).
The American Film Institute ranks her 19th in their list of the top fifty actresses of all time.
Among her many love interests and husbands were the famed director Orson Welles and the Ismaili Prince Aly Khan.
Tragically, Rita Hayworth was diagnosed with Alzheimer’s Disease in 1980. In her case, this is now relayed as a case of so-called “Early-Onset” Alzheimer’s.
This comports with the comments of Hayworth’s daughter Yasmin Aga Khan, who once asserted that her mother had had dementia-like symptoms for “two decades” prior – which, doing the simple math, would have been around 1960, when the actress was in her 40s.
Some researchers now suspect that some forms of Alzheimer’s may be precipitated by various chronic nutritional and vitamin deficiencies. For Hayworth, these may have been bound up with – or at least exacerbated by – habitual alcohol abuse.
She lived with the illness for about seven years after diagnosis, succumbing May 14, 1987 at her home in New York.
Reportedly, she had been in a semi-comatose state since February.
Hayworth’s renown called wide attention to the disease that had been largely ignored or unknown before her diagnosis and death.
Runners Up
Other actors who suffered – or died – from Alzheimer’s Disease include: Raymond Bailey, remembered as Mr. Drysdale, from the popular Beverly Hillbillies t.v. series; 1930s actor Thomas Beck; David Birney, remembered for the 1970s sitcom “Bridget Loves Bernie,” and his relationship with actress Meredith Baxter-Birney; James Doohan, best-known as “Scotty” from the Star Trek franchise; English actress Jill Gascoine, known for the police-themed television show The Gentle Touch; British actor Tony Haygarth; actor Leonard Jackson; lesser-known actor John Kellogg; Jack Lord, best known for his part in the long-running television series Hawaii Five-O; William Marshall, star of the first horror movie (Blacula, 1972) to feature an African-American actor; Simon Scott, known for his rôle in the series Trapper John, M.D.; and film and television actress Stella Stevens.
1. Ronald Reagan
Ronald Wilson Reagan was born in Tampico, Illinois on February 6, 1911. With fifty-three films to his credit, he had modest success on the silver screen.
He was featured in such movies as the 1940 western Santa Fe Trail, with Errol Flynn, …
…and Sam Woods’ 1942 King’s Row – both of which are acknowledged for his respectable acting.
“Ronnie’s” most memorable performance, which earned him the alternate nickname “the Gipper,” was portraying ill-fated college footballer George Gipp in the 1940 biographical film, Knute Rockne, All American.
For the most part, however, Reagan is remembered as a B-movie actor who occasionally veered over into goofball territory, such as with the 1951 comedy Bedtime for Bonzo, where he plays a psychology professor trying to raise and teach a chimpanzee.
Fairly obviously, he is now far more important for his political involvement, which culminated (in 1980) with his election as the 40th president of the United States, than for anything he did while in Hollywood.
That said, it is noteworthy that Reagan transitioned into this phase of his life via two main channels. One was his activity with the Screen Actors Guild, for which he twice served as president.
In fact, when he testified before Congress’s House Un-American Activities Committee, Reagan denounced certain members of the Guild as “Communists.” According to Time Magazine, reporting in 1985, Regean also functioned “…as a secret FBI informant…”.
As the Chicago Tribune stated: “…he and his first wife, actress Jane Wyman, gave the FBI the names of actors who they believed were members of a clique with a pro-Communist line.”
Of course, we previously encountered several actors – including Eddie Albert – who were on the receiving end of such accusations. Mention of Wyman is therefore especially interesting, since you’ll recall that Albert and Wyman worked together on Falcon Crest.
Reagan’s political ambitions were also evident – and probably advanced – in his capacity as spokesman for the multinational behemoth General Electric.
Through his shrewd networking, he became the 33rd governor of California in 1966 (a position he occupied between the powerful family duo of Pat and Jerry Brown). Reagan moved into the White House a few years after his gubernatorial term ended.
During his presidency, Reagan – whether justifiably or not – was credited with reversing the inflation and unemployment (or “stagflation”) that took hold during the 1970s. His laissez faire policies, characterized by reduction of taxes, were collectively called “Reaganomics.”
His ideas – or, at least, those attributed to him – were also termed “trickle-down” theory. The idea was that stimulating large corporations would boost the economy for everyone.
Reagan also increased defense spending and signed an historic treaty with then-Soviet leader Mikhail Gorbachev. The agreement provided that the two large “superpowers” – the United States of America and the Union of Soviet Socialist Republics (or, U.S.S.R.) – would begin to scale back their collections of nuclear weapons.
Reagan’s tenure as president has been cited as priming the U.S.S.R.’s collapse, which unfolded roughly between 1989 and 1992.
In 1994, Ronald Reagan released a dramatic statement beginning with the words: “My Fellow Americans, I have recently been told that I am one of the millions of Americans who will be afflicted with Alzheimer’s Disease.”
Over the next decade, the former “Great Communicator’s” cognitive and physical abilities faded until, June 5, 2004, he succumbed to pneumonia – a common Alzheimer’s-related complication – in his Bel Air home in California.
As a coda, we note that Ronald Reagan had done much during his time as U.S. president to raise public awareness of Alzheimer’s Disease. For example, in 1982, he issued Proclamation 4996, creating a “National Alzheimer’s Disease Week.”
Then, in 1985, Reagan expanded on this with Proclamation 5405, making November “National Alzheimer’s Disease Month” – a commemoration that has continued to the present day.
I have an old video on this topic.
Looking Ahead
Statistical reports suggest that, at present, there are over six million Alzheimer’s sufferers in the United States alone.
According to Alzheimer’s Association projections, that figure is expected to double by the year 2050. Of course, if the number of Alzheimer’s patients increases in the general population, we would expect the same to occur in subgroups. In other words, the number of actors with Alzheimer’s will be going up as well. We’re already seeing indications of this.
Prominent, here, is the Australian-born actor Christopher “Chris” Hemsworth, best known for portraying the Norse demigod Thor in numerous Marvel Cinematic Universe superhero movies.
Recently the press reported that Hemsworth underwent genetic testing as part of a “docudrama” on various aspects of the aging process.
Ultimately, Hemsworth revealed that he possesses two copies of the so-called “Alzheimer’s gene” – one from each side of his family.
Known as the APOE4 gene, it is present in around “in four people. …[B]ut only 2 to 3% of the population have [two copies]…”.
For some context, see the presentation that I did concerning my own test results.
Once again, stay tuned for additional material – both practical and theoretical – that is more central to the channel’s overall theme, which is Alzheimer’s Proofing both your home and your lifestyle.
But if you found something of interest in this video, I ask that you like it. And, if you haven’t already, consider clicking “Subscribe.” Don’t forget to turn on your notifications to be alerted to new content as it becomes available.
Alzheimer’s – and other forms of dementia – are menacing and oppressive diseases.
First and foremost, they take their toll on those who are directly afflicted.
But they can – and do – cause much wider-spread devastation.
Those who have seen it “up close and personal,” know this can include financial, physical, relational, and – for those so-inclined – even spiritual fallout.
I have gotten – and will get further – into those angles in other videos.
But among the myriad negative effects are the various emotional and psychological consequences associated with Alzheimer’s – and with dementia caregiving.
Some of these are widely discussed. At least… they’re addressed in general terms, abstractly.
But there’s an issue that tormented me, personally. Reading comments on some of my videos – especially “When Is It Time For a Nursing Home?” – it seems that I’m far from the only one.
So, in this video, I want to talk about what to do when your caregiving efforts drive you to agonize over the question: Does this make me an awful person?
Caveats
I am not a counselor, psychologist, therapist, or anything close to these. And I am not a healthcare provider or medical practitioner of any kind. Therefore, I cannot diagnose mental- or physical-health conditions, and I am unable to give specific personal advice. If you have depression or thoughts about self-harming or anything in those vicinities, you need to seek professional help. This video is intended for general educational or informational purposes only. I am speaking solely from my own experiences and reflection. And my aim is to raise awareness of these issues as well as foster feelings of solidarity among other caregivers and sufferers. The message is: You’re not alone if you feel this way or have these concerns and doubts.
Ten Reasons Why Being a Caretaker Can Make You Feel Like a Terrible Person
This will be rough-going. I’m going to try (!) not to linger on any point – but just sketch them. As always, your comments are welcomed, especially since it’s a good bet that I missed something.
#1 Missing the Signs of Dementia
If you’re like me, you may have a tendency to punish yourself for not having recognized the evidence of Alzheimer’s, or for misinterpreting the signs that you did see. This may or not be the first thing that prompts you to feel rotten. But, thinking back over my caregiving experience, it was the first thing that I thought of.
As I have explained in several videos, my mom seems not to have recognized my dad’s dementia at all. When I came into the picture, I knew immediately that something was wrong.
But I didn’t understand what I was witnessing. Frankly, I thought my dad had turned into a jerk.
It’s easy to feel bad for thinking ill of him. In retrospect, the temptation is strong to regret not being more intuitive or perceptive or for lack of knowledge.
But REALIZE: Alzheimer’s is a tricky disease. And (as I explained in a past video), even doctors can fail to see the writing on the wall. So don’t beat yourself up! We’re not omniscient, after all.
# 2 Being Unable to Help Them
A major and continual problem is our seeming inability to provide meaningful assistance.
When your loved one is struggling to remember an event or name, you may be unable to convince them of an answer that you know to be correct. And you’ll feel like a failure.
REALIZE: It’s not like helping a non-afflicted person remember something they’ve temporarily forgotten. A normally functioning person can know they’ve forgotten something and, after it’s been brought back to their attention, they can remember what they’re forgotten. Alzheimer’s Disease literally destroys the brain. At some point, a cognitively impaired person may no longer have the forgotten memory or any means to retrieve it.
Even more, we’re powerless to stop the advance of dementia. This is obviously a deeply distressing fact. And even though Alzheimer’s is only one of numerous terminal illnesses, it – and cognitive disorders like it – don’t just kill the body. They kill the mind and the personality.
It’s gut-wrenching when your loved one doesn’t recognize you, or repeats over and over that they wanna go home, when you’ve gone above and beyond to give them a caring environment.
FURTHER REALIZE: That just your calming voice or loving touch is helping them at some level. Yes, you feel terrible when you make a loving home-care environment, but it goes unacknowledged. And, it’s true, once their impairment is far-enough advanced, they probably won’t be able to appreciate your efforts. The most important thing, however, is that you provide an objectively loving, safe, and secured space for them – not that they are aware of your efforts.
#3 Calling in ‘Authorities’
Alzheimer’s sufferers may have outbursts. Some might sob uncontrollably. Others may laugh inappropriately. It’s easy to become distraught when you’re unable to calm or comfort them.
My dad was at the opposite end of the emotional spectrum. He frequently exploded in anger. I had to physically restrain him on one occasion. Just what do you do when things get heated?
I once called a well-known dementia-care support group (that’ll remain nameless). And I asked them this question. Believe it or not, the advice I was given was: Call the police!
…which – after my dad’s next nasty outburst – I actually did.
I’ve no clue whether this suggestion reflected an organizational policy or was just the quirky opinion of the person who happened to answer the phone that day. And I’m not saying the step is never warranted!
But, in my case, the ensuing encounter was thoroughly discouraging – and the intervention was revealed to be obviously unsustainable.
Oh, sure, dad settled down at that moment. But I was made to understand – in no uncertain terms – that the police department had neither the manpower nor the training to be home-care “orderlies.” And it’s not like my dad “learned some lesson” or would even remember the episode.
REALIZE: You do what you can with the data you have. I like to draw an analogy with the daily forecast. If you plan your activities around the expectation of sunny skies – and you did your due diligence: checking the radar and weather report, etc. – and it ends up raining, it’s not your fault. Sometimes the best information available to you is just plain wrong.
Another aspect of this isn’t quite as dramatic. It has to do with your loved-one’s doctor.
As I noted elsewhere, physicians often depend on family members to know that something is wrong with a loved one. In my case, I wrote to my dad’s primary doctor letting him know that my mom, my sister, and I were all extremely worried – especially about the issue of his driving.
Specifically, I had to push the doctor to write a report that resulted in dad’s license being revoked. And that felt really lousy. – like I was going behind my dad’s back and betraying him.
What I had to REALIZE, there, was that other people’s lives and wellbeing were at stake. It wasn’t simply about my dad and his autonomy.
What if he confused the brake and the gas pedal while at our local park? – with families walking everywhere and little kids bike riding, playing, and running all over the place?
No. I felt that – as unfortunate as it was – it had to be done. And, ultimately, it wasn’t me doing anything to my dad; it was the Alzheimer’s Disease that was to blame.
#4 Being Embarrassed by Them
But, of course, when your loved one loses their mobility – or has their autonomy restricted, that doesn’t necessarily mean they simply become homebound shut-ins. – At least, not until the dementia becomes really physically debilitating.
It probably means that you have to pick up the transportational “slack.” And this may not simply range over doctor’s appointments.
If you’re in the position of having to assume caretaking all by yourself – and see my recent video – then you might have to cart them along: As you go shopping and run other household-related or personal errands.
And even if you’ve got help on those fronts, your afflicted loved one will need haircuts. Maybe they gain or lose weight and need to try on new clothes.
You might even want to include them in enrichment or leisure activities. My dad always enjoyed outdoor theater during the summer. My mom and dad had their favorite restaurants. And so on.
But, this can give rise to awkward situations. For instance, I was present at a church service during which my dad caused an obscenity-laced disruption. Several times, he caused a “scene” at local stores. He even picked a fight with a relative during a family reunion over some slight – whether real or imagined – that apparently went back decades.
These sorts of experiences can make you not want to be seen with them in public or take them outside at all.
REALIZE that your loved one may benefit from interpersonal interactions. But, sometimes, events are too busy or loud for a person with dementia. They may easily become overstimulated or overwhelmed. So, if possible, choose events and places that are calm and relaxing.
But what can you do about feeling embarrassed? Firstly, it’s totally understandable. Just ask parents of unruly kids.
Something else that I wish I had done more frequently was to alert people around me about my dad’s cognitive problems. There is one way to do this without making a fuss – and without having to say anything out loud that your loved one might not take well.
Namely, there are little business-card-sized announcements displaying text such as: “The Person I’m With Has Dementia. Please be patient. Apologies for any inconvenience.”
In my experience, most of the time, when bystanders react negatively, it’s because they think that a person who is behaving badly is freely choosing their actions. If you can alert people around that something is wrong, they are often much more forgiving.
#5 Losing Patience With Them
Speaking of this, it’s not always easy for caretakers to remain calm, either. And there’s certainly no shortage of composure-testing situations that can arise in a home-care context.
Providing daily care – including supervision – can become monotonous and tedious. Depending on your demeanor, one of your constant struggles might be losing your temper.
It’s easy to become impatient when you have to say the same things over and over.
Again, child rearing is similar in this regard. But, with kids, at least they’re small and are acquiring the capacities to learn and remember. – Not so with a dementia-afflicted adult.
REALIZE that you might not be able to handle caretaking all by yourself. At some point, you might need to seek assistance. This might mean that you have a heart-to-heart with relatives and ask them to step in – whether temporarily or on an ongoing basis.
But it might also require that you consider professional-care options. As I’ve discussed elsewhere, respite facilities exist to offer family caregivers “breaks” on a short-term basis. And, of course, nursing homes may be the only viable long-term alternatives to home care.
#6 Feeling Your Loved One Is a Burden
Another way to say this might be that you find yourself resenting their decline. I mean…
It’s justifiable, and natural to lament your loved one’s cognitive and physical deterioration.
But what I have in mind is different. It’s that you might find yourself becoming bitter at all the time you have to spend attending to their needs. Or you may develop a “grudge” over the fact that your loved one is unable to appreciate – or understand – your predicament and sacrifices.
Relatedly, you might get depressed – or panicky – at the emotional, financial, or physical strain. This may well include having to take leave from a job and, essentially, to put your life on hold.
REALIZE that you’re only human. Your capabilities and your resources are finite. It’s important – vital even – not to make rash choices. If you find yourself down in the dumps after an especially trying week – or month – then try to give yourself a bit of space.
That’s easier said than done, of course. But, as I have discussed in past videos…
…most recently, the one titled “Is It Possible to Be a Caretaker All By Yourself?” …
…there are a few options available to help you. I’ll defer to some of my other presentations for the details. But you may be able to secure what is called “Respite Care.” This is short-term assistance designed for the sole purpose of giving primary caretakers a much-needed break.
Sidelight: Know (Or Discover) Your Limits
At a certain point in time – it does no good for you to press too far beyond your reasonable limits. I choose my words very carefully. There are three key phrases or terms, there.
“A certain point in time,” “too far beyond,” and “your reasonable limits.”
At the end of the day, only you (and your family) can determine, hopefully in consultation with each other, with friends, and with trusted advisers – like doctors, financial advisers, lawyers, etc. – what these points and limits actually are.
But the flip side of making a hasty decision when you’re temporarily or uncharacteristically emotionally low, is disregarding – or refusing to think about – your limits.
And that can land you in extremely dangerous territory. One sign of this might be, …
#7 Wishing Your Loved One Would Die.
Or wishing that they were already dead. Let’s draw a few distinctions.
Number one, there’s a difference between (on the one hand) lamenting that your loved one is suffering – focusing on their pain for their sake – …
…and (on the other hand) worrying about their pain because of how upsetting it is for you. – whether for you to deal with, or for you to witness at all, or… whatever.
My dad wasn’t diagnosed with Alzheimer’s Disease until the summer of 2009. Immediately preceding that diagnosis, my dad had had two major surgeries just a couple months apart.
On the eve of the first – a triple bypass – my dad was literally on death’s door. Those surgeries prolonged his life for seven years, as it turned out.
But, it’s easy to ask: For what?! Those years were dominated by cognitive decline. I spent four of them caring for him at home, and he spent his last three in a nursing home.
I regularly found myself wishing, or at least, wondering: If only he had died in 2009!
Don’t get me wrong: On my better days, what I was mainly thinking was: If only he had died of a heart attack, his death would have been relatively quick (in theory)… and he would have been spared a near-decade of slowly wasting away – both mentally and physically.
There is space, here, for a discussion of various spiritual perspectives. I’ll leave that complicated topic for a possible, future video. But REALIZE: You can’t control what life gives you; you can only control how you react or respond to it.
Granted, it’s easy to say and hard to do. And I confess: not every thought I had was “altruistic.”
So, number two, we also want to distinguish between a fleeting “bad” thought and an all-consuming idea. Admittedly, there’s a vast middle ground between the two extremes.
Anyone might be susceptible to having the occasional selfish desire. You want to guard against obsessing over such thoughts. For me, this came when my dad was in the nursing home.
Towards the midpoint of dad’s nursing-home stay, we had our first dealings with hospice.
“Hospice” is end-of-life, palliative care for terminally-ill patients. Every time we’d get a call that dad was being “put on hospice,” the news hit us as if he’d just been handed a death sentence. Obviously, I’m speaking loosely. The late-stage Alzheimer’s itself was the real death sentence.
We just didn’t realize that a person can see-saw on and off hospice. Roughly half the time dad was in a nursing home, my family was on edge, expecting that his death might come any day.
That is exhausting, to say the least. Your emotions are like a yo-yo. And it can be both financially and physically demanding.
For example, the first time you think your loved one is at the point of death, you cancel appointments, you take off work, and you otherwise bend over backward to be present as much as possible. If and when they recover, you’re relieved – and not a little surprised, frankly.
But then it happens again. And again. And again. Finally, you worry how you can keep doing this. And you’re basically stuck. If you do react to every wave of hospice as if it were going to be your loved one’s last minutes on earth, then you can place an ever-increasing burden on your family – depending on how many cycles they go through.
After all, it’s not easy to set aside a year, two years, or whatever to be a part of some protracted, open-ended hospice scenario. Sad, but true.
But if you don’t respond, then you risk not being there when your loved one actually passes. You don’t want them to die alone. So, more than once, I wished he would just die. Because I’m here this time. Or my mom is with him right now. Or my sister is visiting from out of town. If he pulls through again, I don’t know which of us will be present next time.
The thing to REALIZE, here, is that we’re only human. The best you can do sometimes, is to take things one day at a time. Have an honest and open dialogue with the hospice and medical staff about your loved one’s situation. And try to plan (as best you can) for rainy-day scenarios.
Regardless of what stage of care you’re in, and where that care is being delivered, try to nip any selfish thoughts in the bud as soon as they pop into your head. Again… easier said than done.
It may help to focus on why you’re doing this. Think about positives – like happy memories. Try to “reframe” the situation, or look at the end-of-life process as a series of opportunities to spend a few more precious moments with your loved one than you thought you’d get.
If you’re in a home-care situation, then consider whether these thoughts – especially if they’re preoccupying you – might be signs of an impending breakdown. Be honest with yourself.
That includes reaching out for help if and when it’s necessary. It might mean that you seek counseling or arrange for respite or hospice care for your loved one.
It doesn’t do any good to simply bury or deny your feelings. The overall caregiving may suffer – which would be bad for your loved one and for you. And that leads to the next consideration.
#8 Regretting Your Caretaking Decisions
It’s an understatement to say it, but …the caretaking road is tiring.
It may also be long and winding. You may feel like you’re wandering lost with no clue how long it will take you to arrive anywhere – or to get back.
You may have mounting debt or expenses. You yourself may be developing age-related physical problems at the same time your loved one is declining. These – and other – factors can lead you to wonder: Can I do this at all? Or …Can I keep doing it?
You can get the distinct impression you’ve bitten off more than you can chew.
And that can lead you to think you made the wrong choice – or a bunch of wrong choices – somewhere along the way. I want to tackle that worry head-on in another video.
But if you start thinking that it was a mistake to take your loved one in, or to assume caregiving responsibilities in the first place, then it can throw you into a spiral of self-doubt.
REALIZE: You’re not alone. Probably every caretaker will harbor similar concerns if they are at it long enough. While this won’t necessarily allay fears that you took a wrong turn, I say it because it’s arguably never clear to anyone what the “correct” path is. You consider your loved one’s well-being of paramount importance, you gather information, you talk your options over with trusted friends and advisers, and you try to do the best you can with the hand you’re dealt.
If, ultimately, things become unmanageable, that may lead to you having to course-correct.
#9 Having to Institutionalize Your Loved One.
And that leads me to this next item. Let me come at this by way of a recent comment. Let’s just say that the opinion was acerbic.
The commenter wrote, in part: “ …I cared for my wife on my own… It did not occur to me to farm her out to await death to make my life more comfortable. …”
Honestly, I doubt that the commenter watched my video. Instead, it seems that he was merely reacting to the title. It’s possible that he misconstrued “When Is It Time for a Nursing Home?” as me saying that – eventually – every caretaking scenario will end with institutionalization. – Which, of course, I don’t believe is true and never said.
Either that, or else he objected that anyone would ever admit their loved one into a nursing home. It’s a view that treats the nursing-home option as tantamount to throwing in the towel (at best) or seeking the easy way out (at worst).
For our purposes, I’m highlighting this because it might easily be taken to heart as an indictment of a caretaker’s commitment to his or her loved one. – As if the only way to show love is to assume full caregiving duties – and stick to them – come hell or high water. Since I turned to professional care, that makes me a bad son.
REALIZE that no one has walked in your shoes. No one should impugn someone’s else’s familial love on the sole basis of their having to utilize a nursing home.
If we didn’t care, we wouldn’t be anguishing over the decision.
But not only is a comment like this uncharitable, it’s really incomprehensible. It half-implies that nursing homes should never be an option.
As many of you know all too well, it’s not always possible – emotionally, financially, physically, or whatever – for family members to be at-home caretakers. In fact, if a better, more complete, kind of care can be delivered in a skilled-nursing facility than in a home, then you could turn the poster’s allegation around and say it would be unloving not to use the nursing home.
Personally, I believe that things are often much more complex and nuanced than either of these dismissive reactions would suggest. For one thing, nursing homes may (or may not) offer quality care. This is just to say that the way forward is not always obvious. In fact, I’d be hard pressed to find a case where the “right decision” is obvious!
No …If there’scertainty in any of this at all, it’s that there is no one-size-fits-all approach.
Thankfully, though, you and I have nothing to prove to anyone else. At the end of the day, it’s for you – in consultation with your support network – to make the best decision you can for your loved one and for your entire family.
#10 Finding That You Don’t Feel Anything at All
Up to now, we’ve been trying to come to terms with various experiences that can make you feel miserable. And that unhappiness can make you wonder if you’re an awful person.
But what happens if you don’t think you’re feeling anything at all?
Someone might hear me explaining how I was tortured over things like the decision to admit my dad into a nursing home or how I was periodically embarrassed by him in public, and so on.
And it’s perfectly imaginable that somebody might think: I’ve never felt anything like that. Does that mean I’m a horrible person?
REALIZE that people deal with adversity differently. I tend to be a reactive, volatile person. I can get worked-up easily.
So, don’t compare – and certainly don’t judge – your emotional reactions to mine or anyone else’s.
But also REALIZE that not feeling anything can mean a lot of different things. For example, it might mean that you’ve become emotionally numb. Caretaker burnout is a real danger.
Remember, also, emotional flatness can be bound up with the so-called “denial stage” of grief processing. So, as I stated earlier, just be willing to be honest with yourself. You might need to take a break. Or you may need professional help – whether for your own mental or physical well-being or for assistance with the day-to-day business of caretaking.
Concluding Remarks
Being a caregiver for someone with dementia can make you feel a lot like Sisyphus. You’ll recall that in the Greek myth, Sisyphus is fated to push a rock uphill for all eternity. Every time he manages to reach the summit, the rock rolls back down the mountain and he has to do it again.
It’s frustrating. It can feel altogether absurd and futile. Additionally, some of the caretaking measures you may need to implement can feel like betrayals. That can be depressing. And it may lead you to feel inadequate, unworthy, and even wretched.
Recently, I realized how many times in past videos I say something like “it sounds bad, but…”.
Why install double-keyed deadbolts on the entry doors? It sounds bad, but… it’s so your loved one can’t easily get out of the house.
How hard is it to care for someone with middle-stage dementia? It sounds bad, but… caretaking can be more manageable if they’re also physically disabled.
I was racked with guilt after having my dad admitted into a care facility. I had nightmares for years afterwards. And it sounds bad, but… the worst were bad dreams in which my dad came back to the house and I was once again thrown into a stomach-churning hopelessness.
You love your afflicted dad, mom, grandparent, spouse, …or child! They’re not actively doing anything to you. They’re not intentionally making you miserable or “oppressing” you.
And you know they’re suffering, too. As my sister said to me during one heart-wrenching exchange in which we discussed institutionalization: Dad is himself in a really bad place.
That’s an understatement, of course.
Trying to imagine what it was like for him is, frankly, sickening. You’re “stuck” inside a body and with a brain that can’t or doesn’t or won’t cooperate with you?! I picture being locked in a windowless room – cut off from others and, eventually, from myself. It’s horrible, hellish, in fact.
Deep down, we know all this “full well,” as the saying goes. That’s the point. The enormity of the pain – on all sides – can be terrifying. Even so, you want so badly to continue to believe that – in their “heart of hearts” – your loved one cares about you, still remembers you, still loves you.
In a sense, it’s precisely that belief – and that hope – that adds insult to injury.
Because… You desperately want to help them. But when they’re cursing you out and throwing things around the house; or when they don’t recognize you and they react to your caretaking as if you were an intruder; or when they refuse to bathe or toilet and you’re routinely cleaning feces off the carpet; you are thoroughly demoralized.
The situation creates an almost impossible tension. You’re sick over the prospect of nursing-home confinement. At the same time, you can feel like you can’t go on and on like this – or you will literally go insane or totally break down physically yourself.
This psychic pressure can build to the point where your mind goes in really dark places.
I’ve been there.
I don’t want to leave this on a negative note.
Please know that I truly, truly, truly empathize.
If you’re presently going through a hard time, then I invite you to share your experiences and thoughts in the comments.
And if you went through a similarly harrowing journey in the past, then I’d ask that you share as well. I have seen really beautiful exchanges in the comments. And I sincerely believe that people who are experiencing self-doubt – or loathing – can benefit from reading about what other people have undergone – and survived.
I hope that – if nothing else – this video encourages you that you’re not alone. And, sometimes, knowing that is about all that keeps you going. I wish you all the best. Thank you for watching.
The easy – and probably unhelpful – answer is: “Sure, it’s possible.” – said, of course, with suitable emphasis on the final word!
After all, anything is supposed to be possible. Right?
But what we’re really asking is: Can I manage it? Will it work in my situation?
And the frustrating reality is, I don’t know.
What I can do is speak from my own experience and research.
But after it’s all said and done, you’ll have to look at this picture, talk it over with family and trusted advisers, and decide whether it would be feasible and realistic for you.
Perhaps the least useless thing I can do is to try to paint a picture of what solo caretaking might look like in the hope that it will give you a framework for your own decision making.
So, strap in, and we’ll start to think through the question: Can you be a caretaker all by yourself?
Preface
I’ll be speaking broadly. I’ll talk about a way solo caretaking could look, drawn from when I was the at-home caregiver for my dad, who died from Alzheimer’s Disease in 2016. I started caring for him in 2008. But we’ll also talk about caregiving variations, based on my research.
The main thing I want to do is to provide you with a blueprint for having a conversation. You will want to talk about possible caregiving scenarios – and pitfalls – with family, friends, and trusted advisers. So, my hope and expectation is that you’ll take what you find useful and leave the rest.
As an “assist,” I’ve prepared a step-by-step guide that you can feel free to download. It’s possible that you can simply Google “Alzheimer’s Proof Caretaker’s Guide.”
But, search engines can be a bit dicey sometimes. So, you can always just point your web browser to AlzheimersProof.com and navigate to it that way.
Introduction
This video was prompted by a viewer-submitted question. As I reflected on the viewer’s situation, one thing I realized is that it is extraordinarily difficult – bordering on being practically impossible – to be entirely solo as a caretaker.
As we move along, it’ll become apparent why I say this. But, what I sincerely hope is that you may also discover, upon reflection, that you’re not actually all by yourself. Or, at least, if you are genuinely alone, then I hope you may come to a deeper understanding of the challenges that lay ahead of you. Not to compound your worries! But simply to enable you to better plan for, and adapt to, circumstances as they arise.
Caretaking Rôle vs. Household Composition
First thing’s first. We should try to clarify what we’re talking about. You’d think that “solo caregiver” is fairly self-explanatory. But I think there are subtleties that need to be made explicit.
What does it mean to be “solo”? There are at least two senses.
‘Solo’ in a Caretaking Sense
Firstly, there’s a caretaking sense. By “caretaking,” I mean assisting your loved one with the Activities of Daily Living (ADLs) – which I explain in a dedicated video – or supervising a cognitively impaired individual, or both.
Just for reference, the basic “ADLs” are: bathing, dressing, eating, maintaining continence, toileting, and transferring (e.g., in and out of bed).
Under the category of “caretaking,” we can further distinguish a primary caretaker from a solo caretaker. Taking the latter first, if you’re a solo caregiver – in a strong sense – then you are the only game in town (or the only player, as it were). It’s entirely and totally up to you – and absolutely no one else – to implement every aspect of your loved one’s care plan.
If you’re a primary caretaker, by contrast, then you have some people in relieving or supportive roles – even if only minimally. Consider a few examples.
Let’s say you have four siblings. One of your siblings drives mom to the doctor’s office. Another buys and delivers her diet-specific groceries and medicine. A third takes her to church on Sunday and spends the day with her. And a fourth can usually be relied upon to fill in for you if you have something come up.
Even so, mom lives in your house. You administer her medicines, prepare her meals, and otherwise tend to her daily needs. You watch her for the majority of the week. The bulk of caretaking duties fall upon you. We might say that you are mom’s primary caretaker.
On the other hand, suppose three of your four siblings live out of state. The other one declines or refuses to help you with any facet of mom’s care. Here, you’re more of a solo caretaker.
Granted, there are cases that are harder to classify. More on that in a moment.
But… it’s not as important to classify the cases as it is simply to recognize that there are different levels of expected responsibility falling on you in each case.
Questions
One of the most pressing questions is: Which case is – or would be – closest to your situation?
Can you expect help with the actual caretaking responsibilities?
At this point, I’m thinking about unpaid help: assistance you’d get from family and (possibly) friends. We’ll consider the role of professionals in a few minutes.
If you’re closer to a primary caretaker, then your questions are things like the following.
How dependable are the secondary caregivers?
Do you have someone who can step in for you in an emergency?
When you get sick, for example, is someone willing to come into your place?
Bear in mind that an Alzheimer’s sufferer may have difficulty adjusting to a new environment. Often, they have enough trouble getting around a familiar place. If the place is comparatively strange, they can be especially difficult to manage.
Do you have a family member willing to be around you when you might be contagious?
Will someone take your loved one to their place for a week?
Remember that the care environment may need to be safeguarded and secured in various ways. I’ve spoken in other videos about many aspects of this. You may need to install childproof locks on cabinets (to prevent your loved one from accessing dangerous chemicals or objects), change thumb-turn locks to double-keyed deadbolts (to reduce the risk of “elopement,” which is the caregiver’s term for when your loved one wanders away from the care environment), install closed-circuit cameras (to monitor them while you do other, necessary work), etc.
Even if you do have a family member who is willing to take dad for a week, it may be necessary for them to prepare their home for this eventuality well in advance.
And if you have no one, how will you function as a caretaker if you are not feeling 100%? What if you become disabled? Etc.
For that matter, how will you sleep? Many of you may realize that Alzheimer’s, and other forms of cognitive impairment and dementia, often interrupt normal sleeping patterns. Usually, this results in an insomnia-type situation at night. Your loved one may have difficulty falling – and remaining – asleep. Sufferers who wake up in the middle of the night may wander. And, unless their environment is entirely free of potential hazards, this nighttime wandering can’t be ignored.
Related questions include: How will you cook or otherwise prepare meals? Similar problems with wandering may appear during the day. If you need time in the kitchen, it may be possible to entice your loved one to join you – possibly by assigning them an easily accomplished or harmless task. But if they refuse to cooperate, or if they start to walk away, you’ll need to make sure they’re not getting into anything dangerous. And that can be easier said than done – especially if the timer’s going off and that dish in the oven is about to burn.
Now… some of these problems lead into another topic.
‘Solo’ in a Housekeeping Sense
Remember I said that there were two relevant senses of the word “solo.” The first was the caretaking sense. The second sense is related – and possibly overlapping.
And that’s the general question of whether you’re alone in your household. Apart from your afflicted loved one, are you literally the only other person in the home?
From this standpoint, we’re talking about whether you’re single, married, or otherwise “partnered”; whether you have kids; whether you have a roommate; or even, in some cases, whether there’s another aging adult that you care for already.
The basic questions, here, are: Are you being helped in running the household? And do you have other people – besides your afflicted loved one – for whom you are responsible?
I want to keep the phrase “running the household” a little vague. After all, this is not a channel about good housekeeping. But, just so we’re on roughly the same page, I have in mind anything – and everything – that goes into making sure the house isn’t condemned and the people inside it don’t starve. Doing chores, paying bills, performing maintenance, and …whatever else.
There are too many household variations to list them all. But we can gesture toward four (4) broad types, under two overarching factors: whether the other people are helping you, or if they’re needing help from you.
Of course, there’s a sense in which any group of people thrown together under the same roof will sometimes help one another and sometimes need help from one another.
But, for this exercise, what you want to ask yourself is: Are the other people in the household helping you in a consistent and meaningful way? Relatedly, you want to ask: Are the other people in the house needing substantial help from you on a regular basis?
We’re going to assume simple “yes” and “no” answers can be given. Real-life cases may involve “maybe” and “sometimes” answers. But… this uncertainty may help you decide what to do.
After all, if your household is already a “question mark” – before you bring in an Alzheimer’s-afflicted loved one – then you might have serious concerns about the viability of a plan that complicates your living situation further.
Ignoring those complexities for the time being, we can arrange the following possible answers.
One case is where you both give help to – and can expect help from – the people in your house. We might think, here, of two married or “partnered” people, for example.
Another is where you provide help, but can’t expect or rely on any in return. An example of this would be a case where you also have young children in the house.
A third is where you don’t really need to provide help, but you still get help. Maybe it’s your house, but one of your grown children lives with you. They pay their own way, as it were, but also do the dishes, maintain your car, mow the grass, etc.
Finally, we can imagine a case where you don’t need to provide much help, but you don’t get much back either. Perhaps you have teenagers. Maybe they’re in college and working part time. They’re starting to pay for necessities and you don’t have to do much for them day to day. But they’re not around much. And they aren’t really contributing to the household.
Some of this will dovetail with financial considerations, which I will say something about in a moment. But, for the time being, and at the risk of harping on the obvious, we can expect that it would be much easier to take on caregiving responsibilities in a household where you’re getting help than one where you’re not getting help.
Likewise, it would be harder to be a caretaker for someone with dementia if you’re also having to provide help to other people already (for example, children).
Still, for all that, it may be possible to add an Alzheimer’s-afflicted loved one into any of the four scenarios. And this is because there are so many factors at play.
For instance, it would make a huge difference if your afflicted loved one presently is in an early-stage – or has a mild form – of dementia as opposed to something more severe.
‘Early’ vs ‘Middle’ vs ‘Late’ Stages
I don’t want this to be a video about Alzheimer’s various stages. I’ve gotten into that topic before – and it may be good to do so again in the future.
At the same time, we can’t avoid touching on the subject, here. But my remarks will be cursory and shouldn’t be taken as a detailed accounting of the progression of dementia.
What I want to highlight is that caretaking challenges are not static. They can and do change – sometimes dramatically, frequently, and unpredictably.
Caveats notwithstanding, we can say that so-called “Early-Stage” Alzheimer’s is characterized by mild difficulties. Memory and reasoning are beginning to be impaired. But this impairment may go unnoticed – even by family and trained physicians.
Possible “comorbidities” aside, your loved one may be able to maintain a large amount of independence. For example, they might be able to cook for themselves, handle basic finances, maintain good hygiene, etc. They might even still be able to drive. Though, this poses special problems and carries risks, as I discuss elsewhere.
From a caregiving perspective, it may not pose insurmountable or even especially difficult challenges to take in a loved one who is in an early stage of cognitive decline. In other words, caregiving – even solo – could potentially be sustained throughout the early stage of dementia.
That said, there are important qualifications. Firstly, given the subtlety of the symptoms, Alzheimer’s may not be diagnosed in its earliest stage. So, families may not be presented with the question of home care until after the dementia becomes more advanced.
I didn’t come in until my dad – by all accounts – was already in Middle-Stage Alzheimer’s.
Secondly, given the current state of the medicine – and enough time – the disease will (unfortunately) progress. This has numerous consequences. Chief among them, for this discussion is that, even if you are able to be a solo caretaker for a while – while symptoms are mild – you have to understand that symptoms will not be mild forever.
If you have a good reason for suspecting that your loved one’s dementia will not become more complicated, that’s one thing. For example, let’s say that your mom is simultaneously (and tragically) diagnosed both with Early-Stage Alzheimer’s and some form of advanced, inoperable cancer. Suppose that her physicians expect her death within 12 to 24 months and they think it likely that she’d still be suffering from only mild dementia during that interval. In that specific case, you’d have good medical reasons for worrying less about how to handle advanced Alzheimer’s than about how best to deliver so-called “palliative care.”
Even so, you may feel more comfortable with a backup plan. After all, the exact progression of the cancer and the dementia are, to some extent, left to the educated guesswork of the doctors. And they are not all-knowing or inerrant.
One final word, here. If Alzheimer’s (or some other dementia) is recognized in an early stage, it may provide a prime opportunity to involve the afflicted loved one in the development of a sustainable, long-range plan for their care. If you simply take them in – and figure you’ll deal with any worsening of their condition later – you may foreclose on that possibility.
Not only this, but if they do live long enough for the dementia to progress, then caregiving will become more complicated. And that is what you can expect by “Middle Stage.”
It’s arguable that Middle Stage is the most difficult, from the standpoint of caregiving in general, and at-home caregiving in particular. Be that as it may, Middle Stage is characterized by a worsening of the pertinent condition. You’ll be dealing with a person who may still be mobile, but who is no longer reliable in terms of decision-making, memory, reasoning, etc.
To put it bluntly: It can be a bit like dealing with a child who has the physical abilities of an adult.
Middle Stage is also often the longest stage. Possibly this is due to the fact that Early Stage may not be detected immediately. Bear in mind that the beginning of “Middle Stage” may not be much worse than the end of “Early Stage.” This might point to the clumsiness or inadequacy of the three-stage view. But my point is that the relevant degeneration and transition can be gradual. The home situation could be fine and manageable until… it’s not.
And – especially if you’re all by yourself – you need to have some awareness of this progression so you can plan accordingly. After all, if it became necessary for you to look into nursing homes, it’s not clear how you would be able to manage visiting and applying to facilities while you’re buried in daily caretaking tasks. And nursing homes almost always have waiting lists.
And while the progression of dementia is somewhat predictable, there are numerous variations.
For instance, Early Stage is usually said to last 1 to 2 years. Fair enough. But you should know that, occasionally, people report a precipitous decline in their loved-one’s cognitive function.
This might occur after a major surgery, for example. My dad took a significant turn for the worse following a triple bypass and a colectomy (spaced out by several months). I’ve seen comments where other people have shared similar stories. It may happen that your loved one is compliant or reasonable one day; then – almost suddenly – they’re obstinate or uncontrollable.
If you can make it all the way to “Late Stage,” you might find that a lot of the Middle-Stage difficulties have subsided. For example, your loved one’s mobility will be drastically diminished. And at a certain point, they will have a near-total impoverishment of their communication ability.
The huge caveat, here, is that Late Stage comes with brand new difficulties. Dealing with a bed- or wheelchair bound person is by no means effortless. They have to be bathed or wiped, changed, fed, hydrated, turned to prevent bed sores. Etc.
When you imagine having to lift an immobile person and help them transfer, you may see why this stage can be extremely physically demanding.
And speaking of those challenges, let’s talk about another set of considerations.
Able-Bodied vs Disabled
Let’s go back to the beginning of the home-care-decision process. Whether the cognitively impaired adult is able-bodied will also matter. Although, this consideration cuts in two directions.
If your loved one has mild-cognitive impairment, then – all other things being equal – it would probably be easier to care for them if they were able-bodied rather than disabled. As stated, many early-stage Alzheimer’s sufferers can perform a lot of daily activities on their own. And while they will need some measure of monitoring and reminding, these kinds of assistance may be “low-impact” and might be manageable by a caretaker who has many other responsibilities.
On the other hand, if your loved one has more severe dementia, then – somewhat paradoxically – it might be easier to care for them (overall) if they were also physically disabled. This sounds bad, but it’s to say that an able-bodied person with significant dementia may be an elopement risk (meaning that they have a tendency to leave the safety of the care environment without the knowledge of the caretaker); or they may otherwise require constant supervision.
I’ve told many stories – in other videos – of times that my dad created messes or safety hazards (whether for himself, for others, or both) in virtue of the fact that he was still ambulatory and mobile, but had lost his ability to recognize perils or to make good decisions.
That said, a severely impaired person who is also disabled may be at increased risk for other things – such as falling. They might fall out of bed, out of a chair or wheelchair, or – God forbid – down a flight of stairs or off the front porch.
To make all this even more complicated, it’s also predictable that – again, all things being equal – a physically disabled person would be more difficult to care for than one who is able-bodied. This is due to the obvious point that a person who is physically disabled will require help getting around, whether to the bath, shower, or toilet; in and out of chairs or bed; or whatever.
Support Network
You also need to consider your – or your loved one’s – support network. And, here, let’s further develop the point – made earlier – that some cases are difficult to classify.
For example, let’s say you’re caring for mom or dad in your home, but that you have siblings who live in the same city. Suppose that they don’t usually assume caretaking responsibilities.
Still, if they could or would assume some responsibilities in the event that you had a personal emergency, you would want to know this – and get that commitment – in advance of needing it.
Is this a case where you’re a primary caregiving, or solo? Once again, and obviously, it doesn’t really matter what you call it. What matters is what help you can rely upon!
I am working on a separate video on talking and planning with family. The best practice is to have hard conversations before emergencies arise. Try to agree on a workable plan in advance.
See, again, the “Caretaking Guide” at AlzheimersProof.com.
Paid vs Unpaid Support
Family can be – and often is – a valuable resource. However, it has its limitations.
What happens if your sister is out of town when you fall ill? She promised to help in the case of an emergency, but she’s just not around.
In such cases, you may need to augment your family network by paying for professional services. So, let’s round out our discussion by picking up the thread I laid down earlier.
There are numerous types of paid services. There may be home-care providers in your area. Some of these may require applications and approvals in advance. This is especially likely if your loved one requires skilled-nursing care, or if you will be – wholly or partially – relying on long-term-care insurance, medicaid, or medicare.
I have a few videos sketching the basics of these. If you would be interested in more, please leave me a comment.
Of course, other options might include changing the care environment altogether. On this wavelength, there are Assisted-Living Facilities and Nursing Homes.
A somewhat middle-of-the-road option would be an Adult Daycare. This is a facility you might be able to utilize alongside home care. For example, maybe you take your loved one to a nine-to-five daycare program Mondays, Wednesdays, and Fridays, but care for them at home the remainder of the week.
A final recourse (still thinking about maintaining homecare) is called Respite Care. Respite Care is designed to give the primary caregiving a short break. But, if the respite provider comes to the home, this may only be for a day or so. If you take your loved one to a respite facility, the respite interval may be a week at most.
For some of the differences in care environments, see my dedicated video. Admittedly, it’s an older video. It might be time to remake it. Feel free to share your opinion in the comments.
Nursing Home
The thrust of this presentation is the feasibility of solo, at-home caregiving. But, what if you determine that it’s simply not feasible?
We should say, emphatically, that it’s not necessary to look at it as an either-or situation.
What I mean is, you shouldn’t think that either you care for your loved one in the home, or else you’re just not involved at all.
When my family made the decision to get my dad admitted to a nursing home, we saw – up close – the level of involvement that he and other patients received from the families.
And it was definitely a spectrum. On the tragic end were those people who received no visits from loved ones. Whether this was because they had no living relatives or because their relatives were unable or unwilling to come, I can’t say. And it probably depended on the case.
In the middle were those people who received regular visits from family members. Maybe it was the same day every week, or always on weekends, or whatever. But these patients had family members who remained involved in their lives.
On the other extreme, there were family members who – barring emergencies and illnesses – came to the nursing home every single day. These devoted folks – whether children, spouses, or whatever – maintained their role as caretakers, despite the change of care environments.
And here’s the crux. You may not be able to accommodate your loved one in your home (or in their home) all by yourself. But you could potentially still be involved as a caregiver – even daily.
I say “potentially,” because (as always) there are complications. For example, it would be an obstacle to daily visits if you had to make a four-hour drive to get to the nursing home. Obviously, all the income-specific considerations are still pertinent, here.
And there are ancillary factors as well. Unless you trust the staff implicitly, or you’re on site frequently, it’s a good idea to vary the days and times of your visits. I will have to get into more detail in another video.
But, in the same vicinity, nursing homes are often understaffed. What staff there is, may be overworked. This may lead to a situation – usually unspoken – where the staff depend upon you to deliver basic care to your loved one. And, well… there’s no delicate way to say this, but: You pay the same for the nursing home whether you are performing caretaking duties or the staff is.
It may come down to the question of whether it matters more to you that your loved one is properly cared for, or whether you get what you (or someone) is paying for.
Financial Considerations
Of course, professional home care, Adult Daycare, Respite Care and the like are not free services. Daycare and homecare can cost several thousands of dollars every month. And if you admit your loved one into a nursing home, the average expected monthly costs start at $4,000.
You or your loved one might qualify – or be able to qualify – for Medicaid. But you should know that not all nursing homes accept Medicaid. Of those they do accept Medicaid, they may not accept it for every available bed in the facility. That is, Medicaid beds may be in short supply.
So the prospect of having – or electing – to pay for care (of any kind) leads immediately into a discussion of finances. …For which – once again – I have dedicated videos.
But… At the most basic level, the question is: What is your financial situation? Among the prominent “sub” questions, here, would be: What is your source of income?
We’d be at it all day if I tried to list all the possible combinations. So, let’s just make a few obvious, summary remarks. If you have to leave the house to go to a 9-to-5 job, then assuming caretaking responsibilities may not be sustainable for you in the long run.
Things might be fine as long as your loved one has mild impairment, is in an early stage, or does not require constant physical assistance or supervision.
But what happens when the dementia advances and becomes more severe? What happens if a fall around the house confines them to a wheelchair? Would you be around them enough every day to notice the sometimes-subtle signs of worsening dementia?
Financially speaking: Could you manage to keep your current job and still be a caretaker?
If your income depends on you commuting to a business, then necessary in-home caregiving will have to be provided by someone else when the time for that comes. Either that or you will have to change your job, take an extended “leave,” or utilize some care facility. As mentioned, Adult Daycare could come into play.
But, what would you do if your loved one is ill and can’t be taken to daycare? Or, what happens if (or when) their dementia advances and they become hard to control or they become ineligible for daycare? Or, what would you do if, as my dad did, your loved one flat refuses to go?
You may be able to cover limited periods of time with paid time off or family medical leave. But at a certain point, your employer may become less understanding. Or corporate policies might demand your termination – regardless of the good will of your immediate supervisor.
If your job is more flexible, or if you work from home, you might have an easier time in some respects. However, even here: How will you ensure that you can devote the necessary time to your job? How will you make sure you have a sufficiently quiet environment in which to work?
It’s not always as simple as giving your loved one an arts-and-crafts project, or hoping they find something to do for a couple hours. What if they become agitated? Would you notice if they wandered off? Do you have some way of monitoring them? – All questions for “9-to-5’ers.”
Finally, a problem may arise more broadly for anyone thinking of taking an extended leave or quitting their current job to be a caretaker. If you’re not actively employed, you might find that some of your benefits – such as your health insurance – will be canceled or suspended. And if you ever found it necessary to rejoin the workforce or to try to get your previous job back, you might find that the position has been eliminated or filled. You might lose seniority. If you have access to a pension, its calculation might be negatively affected by the “lost” years.
There are cases where income may not be an issue for you. One might be if your partner or spouse is the primary breadwinner. Assuming they’re on board with the decision to take in your loved one, then – the idea is – you’d continue relying on their income. No changes. In theory.
Of course, you’ll want to consider whether home care would negatively – and predictably – affect your spouse’s ability to earn a living. If your partner works from home but mom or dad’s raucousness keeps your partner from being able to uphold their job obligations, then things could get messy. What if your loved one has chronic insomnia and their nightly wanderings disturb the whole household? Would your spouse find it difficult to get to the office on time?
Even if things started off “okay,” you’ll want to ask: What happens if the home care starts to interfere with the day job? Will you err on the side of continuing care? Or preserving the job?
These are all genuinely difficult questions.
Other cases of stable income might be ones in which you are able to live off a truly passive income stream – such as guaranteed pensions, royalties, or trust funds.
However, not all “passive income streams” are equal. Some may require periodic tending. Could devote enough time to this maintenance if you were also an at-home caretaker?
Probably the most common case where you may have quasi-dependable income is if you’re fully (not “partly”) retired, and you have unfettered access to all relevant funds (including distributions from 401ks, IRAs, Roth IRAs, dividends, and Social Security).
These can have complications of their own. And it’s beyond the scope of this video to tease out every aspect of relevance. But, if you’re not at least 59 ½, then you likely do not have unrestricted access to retirement funds. And if you’re not at least 62, then you wouldn’t be able to collect Social Security – assuming you’ve qualified for SSA retirement benefits.
Even if you can withdraw money from retirement funds without penalty, you still have to keep an eye on your tax situation. And if distributions from your retirement account depend at all on market performance, then the next economic downturn could upend your ship.
Eventually, if you’re not already doing so, you’ll be forced to take money out of qualified retirement plan accounts by way of the so-called “Required Minimum Distribution.”
The point is that even if you think your finances are “taken care of,” it may not be best thought of as a case of “set it and forget it.”
If you’re living off government assistance, you’ll want to be careful about altering the number of people in the household. Sometimes this can jeopardize your eligibility for some programs.
I can’t and won’t speak to this in any detail, here. Except, I will say that you should consult with experts before finalizing or implementing any changes. And you can see some of my other videos for basic overviews of some relevant programs like Medicaid and Medicare.
It’s worth pointing out that there are a few programs under which you might qualify for government subsidies as a family caretaker. I believe that Medicaid has such a program, sometimes falling under the umbrella of “Consumer Direction.”
Once again, it’s beyond the present scope to detail such a program.
And, of course, eligibility for government programs isn’t the only concern. The amount of assistance you qualify for may change depending on your household’s total financial picture. In some cases, if you change the makeup of the household, you’ll also change that picture.
Obviously, the amount of income is also important for you to reflect on, regardless of its source.
A question would be: Is your current income level sufficient to pay for home-care services – on top of the other, usual household expenses? If not, then it will probably need to be augmented.
Now you might think that if you’re living – or thinking about living – in the same house as your afflicted loved one, then you would have access to their income as well as your own.
And sometimes this is true. But, there are complexities.
I don’t want to make this a video about the relevant ins and outs. However, I could do so if there’s interest. I’m simply trying to bring to the surface issues that may be of relevance.
In that vein, let me just gesture toward some big considerations. As mentioned a moment ago…
Firstly, if your loved one’s income partly consists of government assistance, and is predicated on their living situation, then changing the situation could change the level of assistance. (Boldface, italicize, and underline the word “could.”)
Secondly, be aware that most financial institutions – for example, banks, brokerages, insurance companies, investment houses, retirement-management firms, etc. – are on the lookout for anything that smacks of elder abuse.
If dad’s social-security check suddenly starts getting deposited into daughter’s account; or if mom’s financial adviser or life-insurance agent gets an out-of-the-blue request to “cash out” this or that account or policy; you will probably have to answer some questions before your request or transaction is executed.
This isn’t to say that you’re trying to do anything questionable! Nor is it to say that these kinds of financial requests can’t be honored. But you should be aware that there are levels of legislative protection that have been built into financial regulations over recent decades. And these result in legal “hoops” that sometimes have to be cleared before you can “pool” resources.
Best-case scenario? You’re able to involve your loved one in making all necessary – or desired – changes before their legal or mental competence is undermined (or even called into question).
This might include cashing out or closing some types of account, filling out beneficiary-designation forms, giving you durable or “springing” powers of attorney, opening joint accounts, transferring control or ownership of a financial holding or instrument, and so on.
Once your loved one loses his or her ability to make sound financial decisions, then many – even most (or all!) – of the necessary financial moves you would need to make wouldn’t be advisable (or realizable) without outside authorization. The chief avenue for this would be a conservatorship hearing in a court of proper jurisdiction.
However, appointment as conservator will almost certainly carry restrictions and require reporting to the court. At a basic level, this means that separate bank accounts will have to be maintained, funds shouldn’t be “comingled,” assets can’t be disposed of without court approval, etc. Additionally, conservatorship generally terminates upon the death of the person who was subject to it – so… your loved one. (The subject would be called a “conservatee” or “ward.”)
If your loved one is still able – right now – to converse, decide, and think lucidly on these matters, then you could look into trying to arrange the asset picture in advance of any worsening of their condition. For example, if it is their wish that their financial resources be pooled with yours or otherwise used at your discretion then there is not a moment to lose.
Extremely important caveat! If your loved one is no longer legally or mentally competent, then they are unable to consent to changes to their financial situation. You might face serious – even criminal – consequences even if your loved one’s competency is questionable. All this is beyond me. You’d be wise to consult with legal and medical professionals to ensure that everything is above board. Just to be clear: What I’m saying is for general informational purposes only and should not be construed as any kind of advice.
Suffice it to say… You still do need to be careful with any consolidating moves.
Another point, here. If it’s even possible (that is, conceivable) that your loved one would eventually need Medicaid to help pay for the cost of care, then you have to take great care when assigning, disposing of, gifting, pooling, retitling, selling, or otherwise transferring assets. Because, once again, there are severe repercussions for not following Medicaid’s requirements to a “T.” It took me three dedicated videos just to scratch the surface of Medicaid-related issues.
A Word on Emotions
I’ve been ignoring emotional factors because these are sometimes especially difficult to describe or quantify – partly because they are so bound up with who we are as unique individuals. But, they’re no less an important part of our lives.
You need to consider the emotional impact on – and emotional makeup of – everyone involved.
On the one hand, this means your loved one’s emotions. A diagnosis of dementia would be depressing to anyone with the wherewithal to understand it. It can also be bound up with or give rise to anger, hostility, and resentment.
Alzheimer’s is a mysterious disease. The effects that it can have on emotions are sometimes as puzzling as they are devastating. There is no formula that I am aware of that will predict exactly what you’ll get.
Before his decline, my dad was friendly, likable, and somewhat extroverted. He was also easygoing and, to a large extent, unflappable.
As his cognitive faculties eroded, he became aggressive, belligerent, and combative – with everyone around him. It’s not exactly clear how to understand what occurred.
Did the dementia – so to speak – cause his emotions to “invert”? Did it cause an awakening and overemphasis of dormant negativity? Or did it destroy who he was and, in effect, leave us with someone new?
The other side of the coin, in a solo-caretaking situation, is your emotional tendencies.
If you are mellow and don’t get your feathers ruffled easily, you might be able to take caretaking challenges in stride. On the other hand, if you’re irritable and impatient – like I can be, for sure – then you’re in for an especially tough time.
These considerations need not be determinative or final. Alzheimer’s is always a wild card. And we’re often capable of rising to a challenge. So don’t sell yourself short. Don’t “ostrich” either.
For those who are interested, I dive more into emotional factors in the companion video “Is It Hard to Be a Caretaker?”
Summary Remarks
Okay… this has been a long and bumpy road. Let’s try to take stock.
We started by thinking about what it means to be a “solo” caretaker. We distinguished being a primary caregiver, where others – whether family members or professionals – assist you in backup, respite, and various secondary roles; and being truly solo, where you’re literally handling all caretaking duties by yourself.
But we also noticed that being a solo caretaker doesn’t necessarily mean you’re alone in your home – not counting your afflicted loved one, of course.
It’s difficult to be a caretaker at any level of involvement. It could be a challenge to take dad or grandma for the afternoon, let alone invite them into your house 24/7/365.
If you’re truly going it alone – both as a care provider and as a homemaker – then you’re in for major difficulties. Assuming you have your financial bases covered, however, and you just have to focus on caretaking, I don’t want to say it’s impossible.
Still, you’ll need to have a plan for necessities like cooking, sleeping, and showering – just for yourself. And you’ll probably want to have some sort of lifeline in place if (for instance) you fall ill or become injured. This highlights the need for a viable short-term back-up plan.
This includes numbers for prospective, in-home professional caregivers, Adult Daycares, etc.
Looking farther into the future, you’ll want to have a plan – even if only provisional – for finding a nursing home should that route become unavoidable. This is part of a long-term backup plan.
If you’re more in the primary-caretaker camp, then some pressure might be off of you. But, even so, emotional, medical, and other factors might arise that make it infeasible (or ill-advised) to continue with in-home care.
Additionally, worsening of your loved one’s dementia is, for all intents and purposes, inescapable. Though, of course, it’s possible that a comorbidity might arise and further complicate an already complex situation.
Regardless of your circumstances, you’ll almost certainly run into a situation – probably many – where you’ll need or want professional advice. This could be legal, medical, nutritional, psychological, whatever. You’d be well-served by trying to develop a network of connnexions before your need for expert guidance becomes urgent.
Okay. As difficult as it was to make this video, the really hard part is up to you. You have to reflect on these factors and make the decision. Then you have to put that choice into effect.
Please understand that the Alzheimer’s Proof project – both this channel and the associated website – were designed and intended to help you.
I hope you can turn to some of my resources and find some assistance and value in them.
Finally, let me remind you that I have a second video – written in tandem with this one – which you might find a useful supplement. And don’t forget to check out and download the free workbook that I prepared to walk you through reflecting and choosing a path for your family.
If you’d like to ask follow-ups to me, personally, you can type your comments below or email me at AlzheimersProof@gmail.com.
For legal reasons, I cannot give specific advice. But if there are general concerns, I may be able to speak to them in a future presentation.
Please know that I wish you all the best in this confusing and painful process. Thank you for watching.