So far, most of my content has dealt with Alzheimer’s proofing in home-modification scenarios and other long-term-care conversations.
But, today, I thought I would venture off the beaten path just a little bit.
Alzheimer’s also has a number of interesting theoretical implications as well. My academic background is partly in philosophy and so these theoretical questions are also of interest to me personally.
There are a great number of these cognitive impairments and dementia might surface in a number of different contexts. Ethics is going to be one. Metaphysics is another. Philosophy of mind has obvious relevance. So, I thought I would just pick one of those issues and I decided upon the question of the existence of the soul; that this is an issue that has been debated for thousands of years, so I am under no illusions about trying to resolve the issue in the space of a short web article.
In fact, I am not even going to take sides on the issue, what I want to do instead is just trying to present an accessible introduction to the range of issues, or if you are already familiar with these then call it a refresher course.
The question that is going to be somewhat in focus here is:
Does Alzheimer’s disease disprove the existence of the soul?
What I am going to do is assume the role of the person who says that Alzheimer’s does disprove the soul and then, on the other side of the fence, I’ll play the person who says it does not. I’ll go back and forth like this through five (5) considerations.
But, without further ado, let me present both sides!
Pro and Con Arguments
Against Soul #1: Alzheimer’s is a brain disease that can destroy someone’s personality. That’s the key point.
Alzheimer’s destroys personality by destroying the brain. So, take away the brain, and you take away the personality. A soul simply does not fit into that picture anywhere.
The brain is necessary for personality.
For Soul #1: The brain is necessary for personality. There is no real question about that. So yeah, if you take away the brain, you take away the personality.
But think of a Philly-Cheese-Steak sandwich. If you take away the cheese, you take away the Philly cheese steak sandwich. That does not show that there is nothing to a Philly cheese steak sandwich other than cheese.
The cheese is necessary, just like the brain is necessary. But arguing that the necessity of the brain shows the nonexistence of the soul is like arguing that the necessity of the cheese shows the nonexistence of …bread rolls.
Against Soul #2: Not really, because we already know that bread rolls exist, and we know the full recipe for a Philly cheese steak. It is part of our background information.
But, here, we’re trying to figure out what the full recipe for personality is, based on empirical evidence.
Personality is made up of brain states. Think of it as like how a team is made up of players and coaches. There is nothing more to a team than the people who make it up, and there is nothing more to a personality than the brain states that make it up.
For Soul #2: Well, wait a minute!
The evidence shows dependence. Personality depends on the brain. But dependence is not the same thing as identity.
A team may be identical to the people that make it up. But, then, a team is not a good analogy.
A better analogy would be to think of a musician. A musician depends on a working, well-tuned instrument in order to make music. If the instrument is broken, or out of tune, then the quality of the music is either dramatically lowered, or the musician may not be able to make any music at all. But this dependence of the musician on a working instrument certainly does not imply that music is identical to a good instrument.
Similarly, the fact that personality is dependent on the brain does not mean the two are identical. The brain is an instrument of the soul.
Against Soul #3: But we can experience both musicians and musical instruments. We know they are two separate things because we can have dealings with both of them.
Again, in this case, were trying to figure out how many things there are.
Just because there could be something more than the physical brain does not mean that there is.
Number one, it’s not clear how a nonphysical thing like a soul could use a physical brain as a tool.
And, number two, the principal known as “Occam’s Razor” tells us not to multiply causes, and to prefer simpler explanations.
So, in this case, saying that personality is due to onething – a physical brain – is simpler than saying that it is due to two things – a physical brain plus some mysterious “soul.”
For Soul #3: There’s a saying, sometimes attributed to the famed physicist Albert Einstein: “Make everything as simple as possible, but not simpler.”
Simplicity is great, but it is not always a matter of just counting proposed causes.
Suppose someone is investigating a house fire, and they notice that the wiring is faulty, and that there were oily rags strewn about the entire place.
Now, it would, of course, be simpler to explain the house fire only by talking about the faulty wiring, and not mentioning the oily rags at all. But, if the house fire was in fact caused by faulty wiring and the rags together, then any explanation that leaves one of those factors out is not a good explanation.
Occam’s Razor says we should not multiply causes beyond necessity. Sometimes multiplying causes is necessary.
Against Soul #4: In the case of your fire example, the multiplication of causes is necessary because the scientist, or in that case, the fire investigator, concludes from the evidence that having more than one cause is necessary to give a full explanation.
In the case of personality, the investigators, for example, neuroscientists, have not concluded that we need to appeal to more than the physical brain in order to have an adequate explanation.
So, appealing to anything else simply goes beyond what is needed.
For Soul #4: Fire investigators and neuroscientists are both scientists of nature.
Natural science deals with what is physically measurable and physically detectable.
So, natural scientists can tell you all about the physical causes of physical things, but they cannot tell you about nonphysical things. For example, the fire investigator can tell you about faulty wiring and oily rags but cannot tell you that the fire was a tragedy.
Things like tragedies, or indeed souls, are nonphysical things. But, being nonphysical does not mean that they are not real parts of human experience. They are; they just go beyond what natural science can talk about.
Against Soul #4: We do not need the fire investigator to tell us that the fire was a tragedy. That’s obvious. But having a soul is not obvious.
For Soul #4: Here is what’s obvious: I have a rich inner experience – a private mental life – that goes beyond what neuroscientists can image, or test, or quantify in physical experiments.
Against Soul #5: We are getting off track. Here is the bottom line.
My dad got Alzheimer’s disease and progressively forgot more and more, and got worse and worse until, eventually, somebody could have looked at him and said he was a completely different person.
And that horrible decline was due to a brain disease.
So, at the end of the day, who my dad was, and who we all are, is dependent on, caused by, or explained in terms of the brain.
If something like Alzheimer’s disease comes along and damages our brains enough, it can literally change who we are.
And this is not at all what we would expect if we had, or if we were, something other than, a physical brain.
Therefore, Alzheimer’s disease shows: Probably, there is no such thing as a nonphysical soul.
For Soul #5: Well, my dad went through Alzheimer’s disease, too.
Notice how we both said that.
“Mydad developed Alzheimer’s disease.” “Mydad got progressively worse.” “My dad forgot who he was.”
But all that happened to the same person: My dad.
Yes, his personality was dramatically and tragically changed, because we know – from science – that you have to have a working brain in order to be a healthy and recognizable version of yourself.
But my dad never literally became someone else. If he had, why would the family have continued to care about him at all?
See, that is really the point. If, as I think, he was still numerically one and the same person, even after his brain and his personality were destroyed, then the question is: What was it about them that stayed the same the whole time? What continuous, existing thing explains that identity over time?
It wasn’t his brain, or his memories, or his personality. All those things were destroyed by the Alzheimer’s!
Therefore, I say that the thing that stayed the same was something the Alzheimer’s could not destroy: It was his soul.
Conclusion
These are heavy, theoretical topics! Bear in mind that I have left out quite a lot!
Philosophical reflections on questions regarding the soul may spill over into discussions of personal identity, memory, and so on – each of which on their own fill countless pages and extend back hundreds and even thousands of years.
Conversations of this kind often invoke obscure words and forbidding terminology. You may hear talk of “aboutness” and “intentionality.” You may be exposed to ponderous phrases like “mind-body dualism” and “reductive versus non-reductive physicalism.” You might hear great-big words like “supervenience.”
In the above presentation (and accompanying video!), what I have tried to do is to give a presentation of the issues without any of that jargon.
I have, however, bumped up against some of the deeper concepts. For example, there is an underlying discussion of necessary and sufficient conditions. I touched on this a little bit, without naming it specifically.
But, there are other important issues that I simply haven’t gotten into at all. For instance, there are questions about identity and what is sometimes called “Leibniz’s Law.” I did not really get into those at all.
And the conversation can easily turn into a subset of philosophy called “modality,” where the discussion is about concepts like contingency, possibility, and necessity.
Suffice it to say that there is plenty of room to expand a conversation like this!
So… if you feel like I have left out your favorite argument or your favorite consideration, please understand that I have not done it to purposely weaken one side of the argument or another, or to play favorites. I have simply done it because I felt that introducing another concept might have made the article a little bit less accessible.
And bear in mind that all of that is simply keeping the conversation in the realm of what you might call “philosophy.” The conversation could easily be further expanded to include religious doctrines, theological opinions, etc., and that could be an entire presentation all on its own.
What I did present was simply designed to be an introduction to the issues.
Although I may certainly get into further theoretical issues in the future, understand that this website is mostly about some very practical concerns about how to Alzheimer’s Proof your care environment. Or, indeed, I get into how to Alzheimer’s Proof your own diet and lifestyle to reduce your own risk of developing diseases like Alzheimer’s and other forms of dementia.
Of course, I have further content along those lines planned. So, I invite you to bookmark the page and check back!
Thank you for reading or watching!
Feel free to leave your thoughts in the comments, below.
There are really only three (3) ways to pay for long-term care expenses and nursing costs.
The first general way is with the proceeds from insurance policies. These might be long-term care policies, whether they are qualified policies or non-tax-qualified policies. It could be through short-term care policies; it might even be through hybrid, life-insurance / long-term care combinations.
For people who do not have insurance policies to cover their long-term care costs, the remaining payment options are, second, privately paying from your own income and assets and – for people who do have insufficient income or assets to pay for their care – the final option, third, is applying for government aid. Of course, the most relevant government-aid program is Medicaid.
So, the questions then become: How does one specifically qualify for Medicaid? Or, to put it another way: How does Medicaid determine eligibility?
Caveats
It is important to bear in mind that this is a complex conversation, in part because Medicaid-eligibility requirements are going to vary slightly (and, in some cases, significantly) from state to state. Because of this, you’re going to want to consult with an expert who is knowledgeable about your particular state.
Note: This post tracks along with a YouTube video I have on the same subject.
Medicaid Eligibility
There are two overarching considerations.
Number one, there are financial qualifications.
Number two, there are medical-eligibility requirements.
Most of what I’m going to say is going to have to do with the financial eligibility requirements (because they are so complicated). But let me say a bit about the medical requirements just right off the bat.
Medical Requirements
Generally speaking, Alzheimer’s-level cognitive impairments are going to be enough to qualify you – provided, of course, that they are sufficiently advanced in their severity.
In some literature, you will encounter phrases like “nursing-home-level care.”
The specifics of this are going to vary from state to state. So, once again, you need to seek advice.
However, often, this nursing-home level of care is going to be calibrated to the type of supervision that a person requires, if they have cognitive impairments. Or, it may be calibrated to the various Activities of Daily Living (ADLs) that they are lacking.
Financial Requirements
But what I’m mainly going to be concerned with is going to be the financial eligibility. That’s essentially determined by two (2) calculations or “tests”: an asset test, and an income test.
The question of assets is going to preoccupy us in this article. In a subsequent article, I’ll talk about the income test. (They are both intricate conversations, and so it is probably best to break the conversation up into two pieces.)
Why Are There Financial Qualifications?
The basic reason that these tests exist at all hearkens back to the stated purpose of Medicaid – as I sketched, previously. (For my written article, see HERE; for the companion YouTube video, see HERE.)
In a nutshell, Medicaid provides financial assistance, to help pay medical expenses for people who are impoverished.
And so, the obvious follow-up question is: Who qualifies as “impoverished”?
The answer to that question is determined by these two tests. Basically, the idea is if a person’s assets fall below a certain level, and their income falls below a certain level, then they count as impoverished.
So, as I said: Let’s now consider assets.
Medicaid Asset Requirements
Quick Answer
Essentially, a person has to have $2000 or less in order to qualify for Medicaid, from an asset standpoint.
Two Types of Assets
Now assets themselves are classified into two (2) categories.
The first are “countable assets,” or those that are nonexempt. The second are exemptassets, or those that are not “countable.”
The precise scope of the exemptions and countability will vary from state to state. So, once again, this underscores the need for you to have a conservation with an expert in your area.
Typical Exempt (Non-Countable) Assets
But, usually, an exempt asset is going to be something like these: basic pieces of property, such as the Medicaid recipient’s primary residence,[1]a car, and so on.
Another Caveat
You have to bear in mind that Medicaid can cover people of various ages; it’s not just for people who have Alzheimer’s Disease, dementia, and other cognitive impairments. Medicaid is more broadly applicable than that.
So, for example, it might happen that a 30-year-old Medicaid recipient has a primary residence, has a car, and can get around with no problem.
Now, while it is unlikely – not to say, ill-advised – for a person with advanced Alzheimer’s to be living alone or have a car, those restrictions are not imposed by Medicaid. They are simply result of the advancement of their disease.
What About the Non–Afflicted Spouse?
But the real question occurs when an Alzheimer’s afflicted individual has a spouse who has no affliction. What happens with the assets in that case?
The answer is that the non-afflicted spouse – sometimes referred to as the “noninstitutional spouse,” or the “community spouse” – will also have some assets that are usually going to be exempt.
Those exempt assets will be similar to what was just surveyed for the recipient him- or herself and will usually include a primary residence[2] and a single vehicle.
Medicaid May Seek ‘Recovery’
You should be mindful of the fact that Medicaid will sometimes claim reimbursement for the sale of the home after the Medicaid recipient has died.
You should also be aware that Medicaid is supposed to seek recovery from money that it spends on a recipient’s care.
Because of its strict monetary eligibility requirements, a Medicaid recipient is unlikely to have had any property apart from a home. For this reason, Medicaid often becomes a lien holder against the primary residence, and it may seek to collect money that was generated from the sale of the home.
In a few cases, a home may be required to be sold in order to settle with Medicaid.
However, there are many exceptions to this. In some cases where the noninstitutional spouse or minor child or some other dependent is still living in the home, Medicaid may either be unable or unwilling to seek recovery.
This is complicated territory and, not to sound like a broken record, but you will need to discuss your situation with licensed professionals who are familiar with these kinds of cases.
Countable (Non-Exempt) Assets
For the most part, assets beyond personal effects – like furniture and clothing – will be counted. This includes cash and banking assets, whether they are liquid or “semi-liquid.”
For example, it will include unsettled annuities, bank accounts (like checking accounts, money markets, and savings accounts), as well as certificates of deposit, (or CDs).
Countable assets will also include brokerage and other investment accounts as well as myriad “funds” (such as ETFs, hedge funds, mutual funds, and so on).
It will include cash-value life insurance (whether adjustable life, universal life, whole life, variable life, etc.).
And, importantly, it will include retirement accounts – including 401(k)s and other employer-sponsored defined contribution plans like 403(b)s, 457(b)s, and other employer-sponsored, defined-contribution-type plans. But it will also include Individual Retirement Accounts / Annuities – such as the Traditional IRA and the Roth IRA.
Real-estate and other property, beyond the primary residence and the main vehicle, are also generally non-exempt.
For example, if you have a family cabin or vacation home, then that would be a countable asset.
If you have a boat or a recreational vehicle (RV), then these would be countable assets as well in most cases.
$2,000 Limit
And as I said before, a person having more than $2000 in countable assets will usually be considered (asset) ineligible for Medicaid – although some states like New York have set other asset limits.
What About Property Owned Jointly?
How does it work if assets are shared in common with the spouse?
There are two (2) sorts of state: a “50%” state and a “100%” state.
Each of these types of estates handles assets a little bit differently and I will run through each of these, in turn.
My unofficial count was that approximately 35 states are of the 50-percent type. So, I’ll start with that.
‘50-Percent’ (50%) States
Although the details vary, usually, it happens something like this: All the countable assets are totaled.
So, consider a married couple. Let’s call them “John and Jane.”
The couple’s countable assets will include (1) those that are owned entirely by John, (2) assets owned entirely by Jane, as well as (3) assets that they own together.
The current values or Fair Market Values (FMVs) for these are summed, and then the result is divided by two – hence the name, “50-percent state.”
In general, the non-Afflicted spouse is going to be able to keep half – that is, 50% – of the total, within certain limits.
Two (2) limits are of greatest pertinence: a lower asset limit (or, minimum amount), and the upper asset limit (or, maximum amount).
Minimum & Maximum Asset Limits
These amounts are likely to vary year to year, just like the Internal Revenue Service (IRS) varies the amount of tax deductions, or varies the amount of retirement contributions that you can make.
In 2020, the lower limit was $25,728, and the upper limit was $128,640.[3]
In theory, a person could ask Medicaid to keep an amount outside of those limits. This would be established through a Medicaid “Fair Hearing.” But, in practice, the stated limits are usually final.
50%-State Examples
Case #1
This is complicated stuff, so an example or two might be helpful. I will run through three different scenarios, just for illustration purposes.[4]
Let’s take a middle-of-the-road example to begin.
Step One
Total the assets. Let’s suppose that John’s assets and Jane’s assets, together, are worth $100,000.
Step Two
In a 50% state, we just learned that we take that total and divide it by 2 which (of course) gives us $50,000.
Step Three
Compare the answer to that division problem (the quotient) to the lower and upper limits.
Results
Since our quotient – $50,000 – falls somewhere between the lower limit of $25,xxx, and the upper limit of $128,xxx, in this case, the noninstitutional spouse would get to keep all $50,000.
(This is because $50,000 is less than the maximum-allowable amount, and more than the statutory minimum.)
On the other hand, the institutional spouse, can only have $2000. So, he or she would need to “spend down” $48,000 (on this example), in order to qualify for Medicaid.
(Warning: This is only considering assets! There’s also an income test, as well.)
Case #2
Let’s consider a case now where the assets are a little bit more substantial.
Step One
Let’s suppose that Jane and John both together have $300,000 in assets.
Step Two
Once again, applying the 50% calculation we would take $300,000 and divide it by two. The resultant amount is $150,000.
Step Three
Comparing $150,000 to our stated limits, we notice that it exceeds the 2020 upper limit of $128,640.
Results
This means that, in our second example, the noninstitutionalized spousewillonly be able to keep up to the limit, or $128,640.
As always, the institutionalized spouse can only keep $2000. So, once again, the institutional spouse must spend down the rest of his or her “half.” So… that’s $148,000 (or, $150,000 – $2,000).
But, all the money that is over the limitmust bespent down.
In this case, even the noninstitutional spouse was not permitted to keep the entirety of his or her “half” of the money. So, the noninstitutional spouse must also spend down the remainder of his or her share of the couple’s assets. Here, that amounts to $21,360 (or, $150,000 – $128,640).
Therefore, in this second case, the total spend-down amount is $169,360.
($148,000 from the institutional spouse plus $21,360 from the noninstitutional one).
Case #3
For our third example, let’s consider a case where the assets are far less significant.
Step One
Suppose that Jane and John have a total of $30,000 to their names.
Step Two
When we divide that number by two, we get $15,000.
Step Three
Comparing it to our limits, we observe that $15,000 is less than the minimum amount of $25,728.
Results
That means, in a 50% state, the noninstitutional spouse will get to keep all $25,728, despite the fact that that amount exceeds 50% of the asset total.
On the other hand, since the institutional spouse can only keep $2000, the remaining $2,272 would have to be spent down.
($30,000 of total assets minus $25,728 kept by the noninstitutional spouse minus $2,000 kept by the institutional spouse.)
Takeaway
We see that there is an asset “spend down” that occurs when one’s countable assets exceeds the allowable amounts.
100% States
As I said, not all states operate on a 50% basis. Some are what are called “100% states.” In these states, the noninstitutional spouse may keep all the assets, up to the prescribed limit.
100%-State Examples
In some cases, the practical difference is very slight.
Case #4
Step One
For example, again suppose that Jane and John have $300,000 of total assets.
Step Two
Compare the total assts to stated limits.
Results
In a 100% state, the noninstitutional spouse keeps up to the maximum-allowable amount. In 2020, this is $128,640.
Therefore, the noninstitutional spouse will keep $128,640. This is the same amount that the noninstitutional spouse got to keep in the comparable 50%-state example.
As always, the institutional spouse keeps $2,000, and the rest is spent down.
Case #5
On the other hand, if the assets are less significant, the 100% state approach starts to make a bigger difference.
Step One
So, suppose that Jane and John had a total of $100,000 of assets.
Step Two
$100,000 is less than the 2020 limit of $128,640.
Result
Therefore, in a 100% state, the noninstitutional spouse would keep all $100,000.[5]
Case #6
Step One
Similarly, suppose the assets totaled $30,000.
Step Two
$30,000 is less than the $128,640 limit.
Result
In a 100% state, the noninstitutional spouse would keep all $30,000.
Takeaway
Essentially, in a 100% state, the noninstitutional spouse gets to keep all the assets up to the limit, which is $128,640 in the year 2020.
‘Spend Down’ Doesn’t Mean ‘Give Away’!
Here we run into a potential pitfall.
Upon learning about Medicaid’s austere requirements, and upon surveying their financial situation, couples might be tempted to start giving away assets – whether it be to relatives, to friends or to charities.
This would be a bad idea and very dangerous course of action!
Medicaid’s ‘Penalty Period’
We’ll need to be exceptionally careful.
Medicaid asset transfer rules are every bit as stringent as its other requirements.
Running afoul of Medicaid asset transfer regulations can result in the imposition of what is termed a “penalty.” This is a period of time when the applicant would be ineligible for Medicaid because of procedural violations.
You should also be aware that the penalty period only begins once the applicant would otherwise qualify for Medicaid and often once the applicant is already in a long-term care environment and receiving care.
That means that the Medicaid applicant would be in need of the assistance but would be unable to get it because they are being penalized. In other words, you would be up a creek without a paddle!
The ‘Look-Back Period’
In general, at least for long-term-care scenarios, Medicaid can – and will – review an applicant’s financial history and financial reports going back a full 60 months, or five years.
This “scrutinizing interval” is referred to as the “Medicaid look back.”
What are they looking for?
Medicaid is looking for transfers that are inadmissible from the standpoint of its regulations.
Improper Gifting
Illicit transfers might include things that you might call “improper gifting” and also inappropriate sales.
Illicit gifting would be giving gifts apart from what would be reasonable to celebrate usual occasions (like birthdays and anniversaries) or beyond what would be expected and reasonable in terms of holidays (that is, holidays that your family normally observes).
So, for example, giving little Johnny $50 on his birthday, or buying him a video game might not raise any red flags. (Although, if you are in the process of Medicaid planning, you need to consult with an attorney about every move that you make!)
On the other hand, giving the family cabin to your brother and calling it “an Arbor-Day gift” will almost certainly land you in hot water.
So, don’t make that kind of a mistake!
But, seriously, even inadvertent violations of asset-transfer requirements can be penalized severely.
Your best bet is to consult with an attorney who is knowledgeable about Medicaid transfers.
Firstly, lawyers are liable for the advice that they give to you.
And secondly, it’s against federal law to advise anybody to make asset transfers in such ways to try and hide assets or to cheat Medicaid. If a person’s advice results in the imposition of a penalty, the person giving the advice can be criminally liable.
Caveat
Naturally, this article is not intended to be construed as advice of any kind. It is for general informational, or entertainment, purposes only. You need to consult with experts in your area – perhaps more in this case than others. This is because qualifying for Medicaid is serious business.
Improper Selling
You can get in a lot of trouble, even if you aren’t gifting assets, but if you’re selling them incorrectly.
This is especially the case if the sale price is below the fair market value (FMV) of whatever the item is.
For example, if your car’s blue book value is $10,000. You sell it to your granddaughter for 25 bucks.
This is going to do more than just raise eyebrows. It could get you into a lot of trouble!
Is Every Asset Transfer Illicit?
Now, that isn’t to say that no asset transfers or sales are permissible.
This is an important point because it’s to be expected that a person is transitioning into a new era of their life when going into a long-term care facility, or a nursing home, and they are going to be downsizing, and they’re going to be getting rid of some of their property almost for sure.
The point is that you would be far better getting competent advice when you make these changes, than you would be otherwise.
Permissible asset transfers might include: retitling the home in the name of a spouse or in the name of a caretaking child, or selling items at their fair market value – provided, of course, that the proceeds from the sales are duly noted, tracked, and then reported as part of the countable asset calculation.
Once again, asset transfer rules are state specific, and any Medicaid planning and preparation should be done only under the express advice of an attorney.
Life Insurance
The real difficulty with life insurance is the cash value.
Not every life-insurance policy has cash value. This is going to apply (mainly) to policies that are built on a whole-life or universal-life chassis.
Most term-life policies[6] have no cash value and can (generally) be retained at any face amount.
The “face amount” is the big dollar amount written on the front page of most life-insurance policies. It’s the amount that you would expect to the beneficiary to receive in the event of the insured person’s death.
On the other hand, permanent policies are usually the ones that have cash values. These policies must be limited to $1,500 face values.
That means they can pay out $1,500, at most, in the event that the insured dies. If the face value is $1500, then the cash value is expected to be less than that.
Any contract exceeding these values most likely will need to be “surrendered,” or “cashed out.” (But do not do anything without consulting a competent Medicaid expert or planner!)
Cash-value policies also need to be tracked carefully, even if they are retained.
So, if a policy falls under that $1,500 threshold, it is still going to need to be carefully tracked because: (1) the cash value is still part of the countable assets, and (2) if the policy’s cash value increases or changes year to year, or if the face value goes up, then the policy may qualify this year but not qualify next year.
Final Words
Take a deep breathe.
Because… the income requirements are every bit as complex as the asset requirements!
[1] You should also be aware that there are sometimes limits imposed in terms of how much equity can be inside the house and whether this is applicable or not often depends on whether it is the Medicaid recipient him or herself, who is in the home or whether it is the noninstitutional spouse where equity limits do apply. They tend to vary year to year. In 2020, the amount of allowable equity in a home is about $600,000. Technically about $595,000. In some states it can go all the way up to closer to $900,000 or about $893,000 in 2020.
Intuitively, the reason for the equity limit is so that a person sitting on a $2 million mansion could not qualify for Medicaid when the sale of the home would be enough to discharge both their medical expenses and more modest housing costs. Cases where the spouse is willing in the home equity.
Limits may or may not apply. Consult your Medicaid planner.
[3] These limits may have changed, though; so, don’t too get too hung up on the specific amounts. Just try to get a grasp of the concepts. Your trusted Medicaid expert or planner will be “up” on the relevant limits.
[5] Conceivably, the institutional spouse could keep $2,000 and the noninstitutional could retain $98,000. Consult your Medicaid planner.
[6] Term insurance is usually regarded as “temporary,” since it is purchased for intervals called “terms.” Intervals may be 1 year, 10 years, 20 years, 30 years, etc. The insurance expires if the insured hasn’t died during the interval.
[7] I want to stress that this has been my good-faith effort to provide people with an accessible summary of the contours of Medicaid asset eligibility. However, I make no claims to completeness or expertise. I do not warrant that this information is accurate, error-free, or up to date. So, please, consult with a qualified expert to help you!
Researchers have not yet been able to say definitively what the cause of Alzheimer’s disease is. But, among the candidate causes discussed is oxidation in the body – also called “oxidative stress.”
I want to survey the antioxidant potential of sixteen (16) herbs that you might have on your spice rack at home.
The Relevance of Oxidation
Oxidative stress dovetails with Alzheimer’s disease in several respects.
Firstly, patients who already have Alzheimer’s disease have problems with accelerated oxidation. They have more oxidative stress in their brains.
Secondly, many readers may also be aware that one of the primary characteristics of Alzheimer’s disease is that there is an abnormal accumulation of beta-amyloid and tau protein deposits, which aggregate between – and inside of – nerve cells, gumming up the neural “works.” Well, this abnormal deposition of protein has been speculated either to be the result of an increase in “free radicals” or a decrease in antioxidant defenses inside of some people’s bodies. In other words, it’s the result of oxidation.
But that raises the question: Are antioxidant therapies for Alzheimer’s disease viable?
In attempting to answer this question, we should be mindful of the fact that herbs can be excellent sources for antioxidant. And, as I mentioned at the outset, many of these versatile plants can be found in your kitchen.
In this article, I’ll list sixteen of the most common. (In a follow-up post, I’ll provide a further sixteen that, while less common, are still available.)
Caveats
Obviously, I’m not guaranteeing that you will have all – or even any of – these on your spice rack. Various starter sets will likely include some elements that I don’t write about. Contrariwise, your set may fail to have some component that I do discuss.
Additionally, these profiles are not exhaustive. Moreover, not every example of these herbs will have exactly the same chemical constituents or in the same amounts. It often depends on how the plants are grown, what weather conditions were like, how they were harvested, how the extract was harvested, how was stored, etc. Numerous peer-reviewed scientific journals contain more detailed information on herbs, in general, and on their antioxidant constituents, specifically.
16 Common Antioxidant Herbs You Have on Your Kitchen Spice Rack
Like most of the herbs surveyed here, basil is a good source of vitamins – many of which actually are antioxidants, themselves. But what I’m going to be concerned with is some of the other antioxidant chemicals that are found in these plants.
Basil’s Antioxidant Profile
I have come up with these little graphics with a list of antioxidants. I’m calling these the “antioxidant profile.”
In some cases, an herb’s antioxidant activity can’t be explained solely by the presence of any single compound on the list. In other words, following this line of thinking, it’s not just eugenol, but it’s eugenol in conjunction with all of the other chemicals contained in basil.
(Note: eugenol is more abundantly present in oil of clove. See Part 2.)
This propensity of antioxidants to complement and mutually amplify one another is referred to as “synergism.”
In addition to basil’s significant antioxidants, the herb has also been shown to increase both “memory retention” and “memory retrieval” in experiments on mice.[2]
Spice #2: Bay Laurel Leaves (Laurus nobilis)
Bay Laurel’s Antioxidant Profile
You can see that my list for bay leaves is a little bit less expansive than it was for basil. sale being the primary one.
Nevertheless, bay laurel essential oil is a rich source of natural antioxidants. In fact, the anti-inflammatory and antioxidant potential of “laurel extracts is very significant,” particularly in relation to pathologies such as “Parkinson’s disease, Alzheimer’s disease, and atherosclerosis.”[3]
Spice #3: Black Pepper (Piper nigrum)
Black Pepper’s Antioxidant Profile
This one is really interesting to me. I’m fascinated that this is on the list because even people who don’t have a “collection” of herbs and spices probably have a salt and pepper shaker!
So, it’s amazing that pepper – regular pepper – may have many health-promoting qualities. And it may be highly relevant to Alzheimer’s prevention and treatment.[4]
For example, it’s full of antioxidants.
Piper nigrum’s signature component is something termed “piperine.” You don’t have to go further than the title of one Food-and-Chemical-Toxicology article to get a sense of why this is constituent is so exciting. “Piperine, the main alkaloid of …black pepper, protects against neurodegeneration and cognitive impairment in animal model[s] of cognitive deficit[s] like …Alzheimer’s disease.”[5]
It might be worthwhile to develop a taste for black pepper – if you don’t have one already! Sprinkle a little on your food next dinnertime.
Not only is a good antioxidant, in general, but it actually helps reduce high-fat-intake-induced oxidative stress, specifically.[6] Obesity, and consumption of high-fat diets are both known to be risk factors – that is, increase risk – for Alzheimer’s.
I get into this further in Part 1 of my YouTube-video series on sugar and dementia. (Watch Part 1, HERE.)
But, since black pepper is also purported to have acetylcholinesterase activity,[7]Piper nigrum is also an excellent and promising candidate for multi-target Alzheimer’s-disease therapies.
(And… if you want to get more into acetylcholinesterase inhibitors, I have separate YouTube videos on that subject. For a rudimentary explanation of how acetylcholinesterase inhibitors are supposed to work, see HERE. On the perhaps far-fetched and – as far as I know – merely theoretical possibility that a natural “acetylcholinesterase deficiency” might be beneficial in avoiding Alzheimer’s, see HERE. Finally, on the six, Food-and-Drug-Administration-approved Alzheimer’s drugs – five of which have acetylcholinesterase-inhibiting functions – see HERE.)
It’s worth observing that it’s not just black pepper that is reported to deliver positive health effects. The Piper genus has some 2,000 species of plants.[8] It is plausible to think that at least some of these will have effects similar to those of black pepper just rehearsed.
Spice #4: Cayenne / Paprika (Capsicum annuum)
Cayenne / Paprika’s Antioxidant Profile
Speaking of varieties of pepper, cayenne is another one commonly locatable on kitchen spice racks.
Rich in antioxidants, Cayenne’s main constituents include ascorbic acid, which is (of course) the more “sciency” name for Vitamin C. (By the way, for more on Vitamin C, glance see further down in this article.)
Vitamin C isn’t this pepper’s only arrow in its nutritional quiver. Cayenne also contains a healthy quantity of calciferol, that is, Vitamin D.[9]
Cayenne is known, in part, for is its antidiabetic effect.[10] Of course, diabetes may increase a person’s risk of Alzheimer’s.[11]
I’ll add that some people might have a cannister labeled paprika in their herbal starter packs. Now, I am not a chef, so this is not a culinary observation, but… cayenne and paprika are very similar. In fact, they’re similar enough that, from our standpoint, they can be considered readily interchangeable.[12]
So, for example, paprika is an antioxidant. It contains a variety of compounds, including Vitamin A – or “retinol” – and some other carotenoids, similarly to cayenne. It’s rich in antioxidants.[13]
You can see some validation of this in the article with the somewhat forbidding title, “Binding Antioxidant and Antiproliferative Properties of Sweet Paprika.”[14]
I’ll presently toss in a little caveat. Weather conditions as well as the various, possible ripening stages of individual peppers are going to impact the chemical constituents of these herbs. In the article cited in my footnote, you can see this point in reference to paprika.[15] However, as hinted at in my “disclaimers,” similar statements considerations apply to any of the herbs surveyed.
Cinnamon is loaded with antioxidants, according to the commonly cited website Healthline.[17]
In some ways, cinnamon’s antioxidant effects are similar to those of black cardamom (Amomum subulatum),[18] which I’ll get into in Part 2. (Again, to see this presentation in a YouTube-video format, see HERE.)
Coriander seeds have potential as natural antioxidants.[20] In fact, in addition to coriander’s ability to counteract oxidative stress, the seeds also show antihyperglycemic activity.[21] This makes Coriandrum sativum yet another potential herbal prophylaxis against diabetes. (And this, in turn, may help to reduce a person’s risk of dementia.[22])
Beyond these properties, “Coriandrum sativum seed extract” appears directly relevant to Alzheimer’s and other forms of dementia (for example, Multi-Infarct Dementia, also called “Vascular Dementia”) in virtue of its observed “ameliorative effects on memory impairment in… mice.”[23]
To put it slightly differently, it can possibly “[repair] memory deficits”[24] – which is cause for excitement!
Its constituents include beta-carotene, cineole, and limonene.
According to an article in the peer-reviewed journal Pharmaceutical Biology, cumin also has antistress potential. But, interestingly, especially for the focus of this website, the authors enthuse that cumin also has “memory-enhancing activity.”[26]
They wrote: “This study provides scientific support for the antistress, antioxidant, and memory-enhancing activities of cumin extract and substantiates that its traditional use as a culinary spice in foods is beneficial and scientific in combating stress and related disorders.”[27]
It happens to be an excellent stand-in for coriander. So, if you don’t have coriander seeds, but you do have cumin, you’re in luck. Not only can you expect that cumin is substitutable from a culinary standpoint, but – as alluded to – it also can be used as a stand-in from the standpoint of antioxidant profiles.
Spice #8: Garlic (Allium sativum)
Garlic’s Antioxidant Profile
Speaking of those antioxidant profiles, garlic has a unique one.
Among its noteworthy chemical parts, garlic’s “signature” antioxidant is something called allicin.
Firstly, allicin is being investigated for its possible dual ability to “reduce neuronal death and ameliorate …spatial memory impairment in Alzheimer’s disease models.”[28]
Additionally, allicin also holds promise as an acetylcholinesterase inhibitor[29] – which is the main therapeutic action of the majority of Alzheimer’s drugs – including the preeminent donepezil (sold as Aricept) – currently prescribed.
We already touched on this a bit with black pepper (see above). And we’ll get into it again when we talk about sage (see below), which is also reported to have exceptional acetylcholinesterase-inhibiting activity.[30]
(For my YouTube video on how acetylcholinesterase-inhibiting pharmaceuticals work, click HERE. For my presentation on the six FDA-approved for Alzheimer’s, see HERE.)
In addition to its own antioxidant constituents, Aged Garlic Extract (AGE) has “the ability …to increase the levels of some antioxidant enzymes.”[31]
Among other things, garlic also has a storied history as an antibacterial agent. For more on the herb that, before Alexander Fleming arrived on the scene, was referred to “Russian Penicillin,” see, for example, the article “Extracts From the History and Medical Properties of Garlic.”[32]
Recalling from our discussions of cayenne and cinnamon that diabetes is an Alzheimer’s risk factor, it’s also notable that “[g]inger has been shown to possess anti-diabetic activity in a variety of studies.”[34]
It also turns out that ginger has health-giving properties that are particularly relevant to females of the species. According to the peer-reviewed journal Evidence-Based Complementary and Alternative Medicine: “[G]inger is a potential cognitive enhancer for middle-aged women.”[35]
Finally, for Alzheimer’s, in particular, “Z. officinale may be a promising source of AChE [i.e., acetylcholinesterase – editor] inhibitors for Alzheimer’s disease.”[36] Indeed, some researchers think ginger may spark new insights into multi-targeted pharmaceutical approaches.[37]
Spice #10: Mustard (Brassica nigra)
Mustard’s Antioxidant Profile
It’s easy to dismiss mustard as a mere condiment. But, in fact, “Brassica nigra” is a remarkable “natural food source for antioxidants.”[38]
Healthline elaborates, stating: “Mustard contains antioxidants and other beneficial plant compounds thought to help protect your body against damage and disease. [i]t’s a great source of glucosinolates, a group of sulfur-containing compounds found in all cruciferous vegetables, including broccoli, cabbage, Brussels sprouts, and mustard.”[39]
Its antioxidant profile includes carotenes and kaempferol.
In the article titled “Kaempferol Attenuates Cognitive Deficit Via Regulating Oxidative Stress and Neuroinflammation…,”[40] appearing in the scientific journal Neural Regeneration Research, investigators report “that [kaempferol] may be a potential neuroprotective agent against cognitive deficit in [Alzheimer’s Disease].
As one of the most popular and widely used spices in the world, mustard is readily incorporated into a wide variety of dishes, recipes, and other culinary applications.
That said, however, bear in mind that various mustard-based preparations may include other ingredients besides the bare mustard seeds. Though, admittedly, some of these – for example, turmeric (see my YouTube videos HERE and HERE) and vinegar – may have salubrious properties of their own.
Spice #11: Nutmeg (Myristica fragrans)
Nutmeg’s Antioxidant Profile
Nutmeg is an interesting entrant to this list. First, let’s look at its “pluses.”
Predictably, the stuff “[c]ontains powerful antioxidants.”[41] As Healthline puts it: “Nutmeg contains an abundance of antioxidants, including plant pigments like cyanidins, essential oils, such as phenylpropanoids and terpenes, and phenolic compounds, including protocatechuic, ferulic, and caffeic acids.”[42]
Among its various “catechins,” and other assorted constituents – which together give it a free-radical-scavenging efficiency – is a unique chemical called “myristic acid.”
In one experiment, which involved feeding mice a “ketogenic diet …rich in myristic acid,” the studied diet “…significantly reduced total brain Aβ levels by approximately 25%.”[43]
Of course, the phrase “brain Aβ levels” refers to the pathological accumulation of junk, known as “beta-amyloid protein,” in the brains of Alzheimer’s suffers. These protein deposits are believed by some researchers to be the at-bottom cause of the dread disease. But, the jury is still out.
(For my own discussions of candidate Alzheimer’s-Disease causes, I invite you to see my WRITTEN ARTICLE elsewhere on this website or, if you’d prefer, view one of my early YOUTUBE-VIDEO efforts.)
Now… onto a few significant “minuses.”
In a New York Times article titled “A Warning on Nutmeg,” the author points us to the historical fact that, “[i]n the Middle Ages, it was used to end unwanted pregnancies.”[44]
This past employment as an herbal abortifacient would probably be little more than a footnote, were it not for the fact, reported by the Journal of Medical Toxicology, that there is such a thing as “nutmeg poisoning.”[45]
And this leads us to the somewhat darker side of nutmeg’s properties: myristicin’s potentially toxic effects.[46]
The concern shouldn’t be overstated, however. These poisoning cases are rare. They tend to involve teenagers horsing around. So, you don’t necessarily have to worry – for example, if you’re following quantity information in a tried-and-true recipe.
Still, interested persons should proceed with caution, since there’s little to go on in terms of precise information regarding how much nutmeg may be needed to cause some of the nastier effects (like hallucinations, nausea, and vomiting).
The New York Times says: “It takes a fair amount of nutmeg — two tablespoons or more — before people start exhibiting symptoms.”[47] That quantities of this sort (two tablespoons or more) are required is underscored by some of the poisoning reports available.[48]
Healthline suggests that doses can be less and still result in adverse events. In the article “High on Nutmeg,” writer Eleesha Lockett tell us: “According to the case studies from the Illinois Poison Center, even 10 grams (approximately 2 teaspoons) of nutmeg is enough to cause symptoms of toxicity. At doses of 50 grams or more, those symptoms become more severe. Like any other drugs, the dangers of nutmeg overdose can occur no matter the method of delivery.”[49]
Just handle nutmeg with care. For example, use only as directed by trusted recipes, and keep it out of reach of kids, teenagers, and the cognitively impaired.[50]
A glance at my “profile” for oregano reveals a plethora of powerful, constituent antioxidants, including rosmarinic acid – a compound also found in lemon balm (Melissa officinalis), peppermint (Mentha × piperita), rosemary (Rosmarinus officinalis), sage (Salvia officinalis), and thyme (Thymus vulgaris) – and which, in addition to its antioxidant capabilities, “…possesses many biological activities including …anti-inflammatory, anticancer, antiviral, antibacterial, and neuroprotective effects.”[52]
“Dietary intake of oregano oil has been reported to significantly delay lipid oxidation in animal models…”.[53]
One Science Daily post humorously puts things this way: “In what may be good news for pizza lovers and Italian-food connoisseurs everywhere, the herbs with the highest antioxidant activity belonged to the oregano family. In general, oregano had 3 to 20 times higher antioxidant activity than the other herbs studied,” according to at least one American-Chemical-Society investigation.[54]
Rosemary has “potent antioxidant properties” which “have been mainly attributed to its major diterpenes, carnosol and carnosic acid, as well as to the essential oil components”[55] – names for some of which you can read on the “dossier” that I have prepared.
We looked at another, characteristic antioxidant component – namely, rosmarinic acid – when we covered oregano, above.
Rosemary is quite noteworthy. In fact, I have two video presentations dedicated to it (viewable HERE and HERE), including one (ßthe second link!) where I (unofficially!) name it my pick for the second-best “Alzheimer’s herb” – just behind Gingko biloba.
Suffice it to say that rosemary is one of those “powerhouse” herbs that appears to be capable of attacking Alzheimer’s from multiple angles, including: providing “…general antioxidant-mediated neuronal protection,” guarding against “brain inflammation,” and even possibly hindering “amyloid-beta (Aβ) formation.”[56]
(Recall that nutmeg was alleged to have a similar, Aβ-inhibiting action. For a review, see the relevant section, above. And, for similar remarks about sage, continue, below!)
Spice #14: Sage (Salvia officinalis)
Sage’s Antioxidant Profile
As Healthline puts it: Sage is “Loaded With Antioxidants”![57] In fact, the herb reportedly “…contains over 160 distinct polyphenols, which are plant-based …antioxidants…”.[58]
Like oregano and rosemary before it, sage also contains nonnegligible quantities of rosmarinic acid (see the writeup on oregano for details). But it also has salvianolic acid, a chemical that is somewhat unique to Salvia plants.
The widely studied Red-Sage species, Salvia miltiorrhiza, for example, has “Salvianolic acid B (Sal B),” a “major and …active anti-oxidant …[that] protects diverse kinds of cells from damage caused by a variety of toxic stimuli.”[59]
Though, I hasten to add that “…salvianolic acid” shows up as one of the “major components” in “…analyzed samples of S. officinalis…,” or garden-variety sage, as well.
The remarks made in one scientific article are worth quoting at length.
“Amongst many herbal extracts, Salvia species are known for the beneficial effects on memory disorders… S. officinalis (common sage), Salvia lavandulaefolia (Spanish sage), and Salvia miltiorrhiza (Chinese sage) have been used for centuries as restoratives of lost or declining mental functions such as in Alzheimer’s disease (AD).
“…In AD, the enzyme acetyl cholinesterase (AChE) is responsible for degrading and inactivating acetylcholine, which is a neurotransmitter substance involved in the signal transferring between the synapses. AChE inhibitor drugs act by counteracting the acetylcholine deficit and enhancing the acetylcholine in the brain. …Essential oil of S. officinalis has been shown to inhibit 46% of AChE activity at a concentration of 0.5 mg/ml.
“…A study shows that S. officinalis improves the memory and cognition… A randomized, double-blind clinical study has shown that an ethanolic extract from common sage (S. officinalis) as well as Spanish sage (S. lavandulaefolia) is effective in the management of mild to moderate AD…”
“…The cytoprotective effect of sage against Aβ (amyloid-beta plaques) toxicity in neuronal cells has also been proven by …a study which provides the pharmacological basis for the traditional use of sage in the treatment of AD.”[60]
Therefore, sage – along with other plants like gingko, rosemary, and saffron – belongs high on any list of possible herbal Alzheimer’s interventions.
Let me interject, at this point, that if you want more detailed information on or about any of these herbs, then I would invite you to do a little bit of research yourself on PubMed.
First of all, many articles specify more of the antioxidant constituents than I do.
Secondly, as just illustrated by the previous, long quotation, numerous scholarly articles excavate the therapeutic potential of these spices much more completely – and expertly – than I can do in this space.
(However, for a nontechnical introduction, I invite you to check out my own treatment of sage on YouTube, HERE.)
(For a refresher regarding the significance of this activity for Alzheimer’s Disease, see the entries for black pepper and garlic, above. See also: my YouTube presentations on the function of acetylcholinesterase inhibitors, HERE; hypothetical “acetylcholinesterase deficiency,” HERE; and FDA-approved Alzheimer’s drugs which have acetylcholinesterase-inhibiting functions, HERE.)
Spice #15: Thyme (Thymus vulgaris)
Thyme’s Antioxidant Profile
Regarding thyme, one website reports: “It turns out that this useful kitchen herb is also a high-antioxidant food.”[61]
In fact, thyme – or, at least, its essential oil – is arguably one of the most potent herbal antioxidants. One set of authors reports: “The best antioxidant[62] was T. vulgaris oil.”[63]
And among thyme’s most important constituents – a summary of which you can see in the “profile” that I prepared – is thymol, itself one candidate (on a short list) for the title most powerful antioxidant.
One journal states: “Thymol, carvacrol, and eugenol are the most powerful antioxidants…”.[64]
Thymol is so potent that even “waste thyme extract can… be used as an antioxidant either in food or pharmaceutical emulsions…”.[65]
In terms of Alzheimer’s-Disease relevance, I note that “…thymol decreased the effects of Aβ on memory and could be considered as neuroprotective.”[66]
On top of all this, thyme also displays antimicrobial properties.[67]
(For more on thyme, including a segment on borneol (a constituent that is able to improve the transportation of other therapeutic compounds into the brain) see the YouTube version of this presentation, HERE.)
Spice #16: Turmeric (Curcuma longa)
Turmeric’s Antioxidant Profile
This herb is more widely known – and regarded – for its potent anti-inflammatory properties.[68]
But, make no mistake, “[t]urmeric is a powerful antioxidant,” also.[69]
The key component is something called “curcumin.” Now, the relationship between curcumin and turmeric is a bit tricky, especially when it comes to supplements. Curcumin has been thoroughly studied for its health benefits – which are numerous.
But, by itself, curcumin does not have the same health benefits from a practical standpoint, because it doesn’t get absorbed well in the digestive tract.
An article in USA Today makes the point.
“Curcumin is a nutritional compound located within the rhizome, or rootstalk, of the turmeric plant. An average turmeric rhizome is about 2% to 5% curcumin. …[I]t’s the curcumin …that has the powerful health benefits. …You would have to take hundreds of [turmeric] capsules to get a clinically studied amount of curcumin. …[But p]lain curcumin extracts are poorly absorbed in the intestinal tract.”[70]
Synergy
One possible workaround arguably depends upon the concept of synergism – mentioned earlier. Recall that this has to do with the idea of “combining” or “pooling” potencies.
So, for example, curcumin can be taken with another of turmeric’s constituents, namely, aromatic turmerone, sometimes abbreviated as “ar-turmerone.”[71]
Another possibility is a combination of curcumin and black pepper, the common spice discussed earlier in this article. “[P]iperine is the major active component of black pepper and, when combined in a complex with curcumin, has been shown to increase bioavailability by 2000%.”[72]
A further illustration of the power of synergy is offered by the Journal of Agricultural Food Chemistry, where we read the following. When sage and thyme are combined, antioxidant constituents, including “[c]arnosol, rosmanol, epirosmanol, isorosmanol, galdosol, and carnosic acid” together “exhibited remarkably strong activity, which was comparable to that of alpha-tocopherol.”[73]
“Alpha-tocopherol is the most active form of vitamin E in humans.[74] It is also a powerful biological antioxidant. Vitamin E supplements are usually sold as alpha-tocopheryl acetate, a form that protects its ability to function as an antioxidant.”[75]
Blends
And… don’t forget about spice blends! Many blends provide you with these common herbs in combination.
For instance, curry powder frequently includes ingredients such as coriander, fenugreek, ginger, and – of course – turmeric.
Chili powder might have garlic in addition to cayenne or paprika.
Italian-seasoning blends are typically going to include basil, garlic powder, oregano, Rosemary, thyme, and so on. Sometimes there’s an assist from things like marjoram or parsley – both of which I get into in part 2. (See HERE.)
There are a number of other blends, of course. For example, there’s poultry seasoning, which can have oregano, sage, and rosemary, but also secondary constituents like black pepper and marjoram.
My point in mentioning blends in these cursory comments is simply this.
Even if you look at your spice rack see discover that you don’t have most – or any – of the sixteen herbs expressly named on my list, if you have a few blends, you might find that you have more than you think you do.
Vitamin C
As a coda, I’ll add that many – in fact, nearly all – of these herbs also include vitamins. In conversations about antioxidants, one of the most significant vitamins is Vitamin C, or ascorbic acid.
Take thyme, for example. Thyme is frequently touted as a significant source of vitamin C. In its article “20 Foods That Are High in Vitamin C,” Healthline reports that “[o]ne ounce (28 grams) of fresh thyme provides 45 mg of vitamin C, which is 50% of the D[aily]V[alue].”[76]
Of course, you’re probably unlikely to consume that much thyme at one sitting.
Moreover, note that the article in question specifically mentions fresh thyme – as opposed to the dried stuff. It’s arguable that fresh herbs are often higher than their dried counterparts in terms of vitamin content, but lower in terms of other antioxidants – or, at least, in terms of measured, overall antioxidant potency.[77]
(I plan on tackling the vexed topic of “ORAC values” in another place.)
Bottom line: just be aware that many of these herbs can deliver some vitamin content. In fact, every one of the herbs that I survey, here, is reported to have some Vitamin-C content.
For More Information
Where can you go for more?
PubMed is a publicly searchable database of scholarly articles, many of which (though, not all) are posted in full-text format. Just use search strings such as <“antioxidant” + [your favorite herb]>. PubMed is accessible, HERE.
Among the numerous, informative articles that you may find is an offering like this: “Antioxidant Activity of Spices and Their Impact on Human Health: A Review.”[78]
That article is actually published by the international, peer-reviewed, academic journal Antioxidants – located HERE – which, as its name suggests, focuses on the topic that has occupied us in this post.
Additionally, though, my website and YouTube channel are sources for basic introductions to many topics in the vicinity. Some of the titles that readers may find interesting include:
All 25 of the herbs in the three installments just mentioned appear in a written article on my website, available HERE.
Finally, I’ll mention my YouTube presentation on “Rosemary” (a dedicated, early video I made on this spice)
[By Matthew Bell]
Notes:
[1] Basil is sometimes referred to as “Sweet Basil.”
[2] Shadi Sarahroodi, Somayyeh Esmaeili, Peyman Mikaili, Zahra Hemmati, and Yousof Saberi, “The effects of green Ocimum basilicum hydroalcoholic extract on retention and retrieval of memory in mice,” Ancient Science of Life, vol. 31, no. 4, Apr.-Jun. 2012, pp. 185-189, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3644756/>.
[3] According to: Biljana Kaurinovic, Mira Popovic, and Sanja Vlaisavljevic, “In Vitro and in Vivo Effects of Laurus nobilis L. Leaf Extracts,” Molecules, vol. 15, no. 5, May 2010, pp. 3,378-3,390, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6263372/>.
[4] For just one hint of this, see: Lokraj Subedee, R. Suresh, M. Jayanthi, H. Kalabharathi, A. Satish, and V. Pushpa, “Preventive Role of Indian Black Pepper in Animal Models of Alzheimer’s Disease,” Journal of Clinical and Diagnostic Research, vol. 9, no. 4, Apr. 2015, pp. FF01-FF04, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4437082/>.
[5] Pennapa Chonpathompikunlert, Jintanaporn Wattanathorn, and Supaporn Muchimapura, “Piperine, the main alkaloid of Thai black pepper, protects against neurodegeneration and cognitive impairment in animal model of cognitive deficit like condition of Alzheimer’s disease [sic],” Food Chem. Toxicol., vol. 48, no. 3, Mar. 2010, pp. 798-802, < https://pubmed.ncbi.nlm.nih.gov/20034530/>.
[6] BrahmaNaidu Parim, Nemani Harishankar, Meriga Balaji, Sailaja Pothana, and Ramgopal Rao Sajjalaguddam, “Effects of Piper nigrum extracts: Restorative perspectives of high-fat diet-induced changes on lipid profile, body composition, and hormones in Sprague-Dawley rats,” Pharmaceutical Biology, vol. 53, no. 9, Apr. 9, 2015, pp. 1,318-1,328, <https://pubmed.ncbi.nlm.nih.gov/25856709/>.
[7] Kazuya Murata, Shinichi Matsumura, Yuri Yoshioka, Yoshihiro Ueno, and Hideaki Matsuda, “Screening of β-secretase and acetylcholinesterase inhibitors from plant resources,” Journal of Natural Medicines, vol. 69, no. 1, Aug. 15, 2014, pp. 123-129, <https://pubmed.ncbi.nlm.nih.gov/25119528/>.
[8] J.D.D. Tamokou, et al., “Antimicrobial Activities of African Medicinal Spices and Vegetables,” Victor Kuete, ed., Medicinal Spices and Vegetables from Africa: Therapeutic Potential against Metabolic, Inflammatory, Infectious and Systemic Diseases, London: Academic Press; Elsevier, 2017, p. 223, <https://books.google.com/books?id=SHjUDAAAQBAJ&pg=223>.
[9] Cholecalciferol, also known as Vitamin D3, is a particularly highly regarded variety.
[10] Setareh Sanati, et al., “A Review of the Effects of Capsicum annuum L. and Its Constituent, Capsaicin, in Metabolic Syndrome,” Iranian Journal of Basic Medical Sciences, vol. 21, no. 5, May 2018, pp. 439-448, <https://pubmed.ncbi.nlm.nih.gov/29922422/>.
[12] Arguably, they’re literally identical. At least, in some preparations, they seem to be the same herb. But, since I am not experienced enough to know whether this is the usual state of affairs, I’ll stick to the more reserved word, and simply say that they’re similar.
[14] Hong-Gi Kim, et al., “Binding, Antioxidant and Anti-proliferative Properties of Bioactive Compounds of Sweet Paprika (Capsicum annuum L.),” Plant Foods for Human Nutrition, vol 71, no. 2, Jun. 2016, pp. 129-136, <https://pubmed.ncbi.nlm.nih.gov/27184000/>.
[15] F. Márkus, H. Daood, J. Kapitány, and P. Biacs, “Change in the carotenoid and antioxidant content of spice red pepper (paprika) as a function of ripening and some technological factors,” Journal of Agricultural Food Chemistry, vol. 47, no. 1, Jan. 1999, pp. 100-107, <https://pubmed.ncbi.nlm.nih.gov/10563856/>.
[16]Cinnamomum verum is sometimes designated “Ceylon Cinnamon.” It is a close cousin to the Chinese variety, Cinnamomum cassia, which is more commonly found on grocery-store shelves. According to an article in the Wall Street Journal, C. verum is considered safer than C. cassia – at least in high doses. Additionally, C. verum is assumed to share many of the same salubrious properties of C. cassia, which latter has (admittedly) been more thoroughly studied in scientific experiments. See Laura Johannes, “Little Bit of Spice for Health, but Which One? While Ceylon Cinnamon Is Milder Than Grocery-Store Variety, There Are Few Studies on Its Benefits,” Wall Street Journal, Oct. 14, 2013, <https://www.wsj.com/articles/little-bit-of-spice-for-health-but-which-one-1381786452>.
[18] J. Dhuley, “Anti-Oxidant Effects of Cinnamon (Cinnamomum verum) Bark and Greater Cardamom (Amomum subulatum) Seeds in Rats Fed High-Fat Diet,” Indian Journal of Experimental Biology, vol. 37, no. 3, Mar. 1999, pp. 238-242, <https://pubmed.ncbi.nlm.nih.gov/10641152/>.
[19] Just a terminological note: Coriander and cilantro are the same plant, Coriandrum sativum. Some people, in some contexts, probably use the words “coriander” and “cilantro” as synonyms. But the way I’m using these words is this. “Coriander” refers to the seeds of the plant, whereas, “cilantro” refers to the aerial parts (leaves, etc.).
[21] B. Deepa, C. Anuradha, “Antioxidant potential of Coriandrum sativum L. seed extract,” Indian Journal of Experimental Biology, vol. 49, no. 1, Jan. 2011, pp. 30-38, <https://pubmed.ncbi.nlm.nih.gov/21365993/>.
[22] For just one report on this, see: Ramit Ravona-Springer and Michal Schnaider-Beeri, “The association of diabetes and dementia and possible implications for nondiabetic populations,” Expert Review of Neurotherapeutics, vol. 11, no. 11, Nov. 2011, pp. 1,609-1,617, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3240939/>.
[23] Yurina Mima, Nobuo Izumo, Jiun-Rong Chen, Suh-Ching Yang, Megumi Furukawa, and Yasuo Watanabe, “Effects of Coriandrum sativum Seed Extract on Aging-Induced Memory Impairment in Samp8 Mice,” Nutrients, vol. 12, no. 2, Feb. 11, 2020, pp. 455ff, <https://pubmed.ncbi.nlm.nih.gov/20848667/>.
[25] N. Thippeswamy and K. Naidu, “Antioxidant potency of cumin varieties—cumin, black cumin and bitter cumin—on antioxidant systems,” European Food Research and Technology, Jan. 12, 2005, vol. 220, pp. 472-476, <https://link.springer.com/article/10.1007/s00217-004-1087-y>.
[26] Sushruta Koppula and Dong Kug Choi, “Cuminum cyminum extract attenuates scopolamine-induced memory loss and stress-induced urinary biochemical changes in rats: a noninvasive biochemical approach,” Pharm. Biol., vol. 49, no. 7, Jul. 2011, pp. 702-708, <https://pubmed.ncbi.nlm.nih.gov/21639683/>.
[28] Xian-Hui Li, Chun-Yan Li, Zhi-Gang Xiang, Fei Zhong, Zheng-Ying Chen, and Jiang-Ming Lu, “Allicin can reduce neuronal death and ameliorate the spatial memory impairment in Alzheimer’s disease models,” Neurosciences (Riyadh, Saudi Arabia), vol. 15, no. 4, Oct. 2010, pp. 237-243, <https://pubmed.ncbi.nlm.nih.gov/20956919/>.
[29] Suresh Kumar, “Dual inhibition of acetylcholinesterase and butyrylcholinesterase enzymes by allicin,” Indian Journal of Pharmacology, vol. 47, no. 4, Jul.-Aug. 2015, pp. 444-446, <https://pubmed.ncbi.nlm.nih.gov/26288480/>.
[31] Ana L. Colín-González, Ricardo Santana, Carlos Silva-Islas, Maria Chánez-Cárdenas, Abel Santamaría, and Perla Maldonado, “The Antioxidant Mechanisms Underlying the Aged Garlic Extract- and S-Allylcysteine-Induced Protection,” Oxidative Medicine and Cellular Longevity, vol. 2012, 2012, p. 907,162, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3363007/>.
[32] Biljana Petrovska and Svetlana Cekovska, “Extracts from the history and medical properties of garlic,” Pharmacognosy Review, vol. 4, no. 7, Jan.-Jun. 2010, pp. 106-110, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3249897/>.
[34] Nafiseh Khandouzi, Farzad Shidfar, Asadollah Rajab, Tayebeh Rahideh, Payam Hosseini, and Mohsen Mir Taherif, “The Effects of Ginger on Fasting Blood Sugar, Hemoglobin A1c, Apolipoprotein B, Apolipoprotein A-I and Malondialdehyde in Type 2 Diabetic Patients,” Iranian Journal of Pharmaceutical Research, vol. 14, no. 1, Winter 2015, pp. 131–140, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4277626/>.
[35] Naritsara Saenghong, et al., “Zingiber officinale Improves Cognitive Function of the Middle-Aged Healthy Women,” Evid. Based Complement Alternat. Med., vol. 2012, Dec. 22, 2011, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3253463/>.
[36] Bui Thanh Tung, Dang Kim Thu, Nguyen Thi Kim Thu, and Nguyen Thanh Hai, “Antioxidant and acetylcholinesterase inhibitory activities of ginger root (Zingiber officinale Roscoe) extract,” Journal Complementary and Integrative Medicine, vol. 14, no. 4, May 4, 2017, <https://pubmed.ncbi.nlm.nih.gov/29345437/>.
[37] See: Faizul Azam, Abdualrahman Amer, Abdullah Abulifa, and Mustafa Elzwawi, “Ginger components as new leads for the design and development of novel multi-targeted anti-Alzheimer’s drugs: a computational investigation,” Drug Design, Development and Therapy, vol. 8, 2014, pp. 2,045-2,059, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4211852/>.
[40] Somayeh Kouhestani, Adele Jafari, and Parvin Babaei, “Kaempferol attenuates cognitive deficit via regulating oxidative stress and neuroinflammation in an ovariectomized rat model of sporadic dementia,” Neural. Regen. Res., vol. 13, no. 10, Oct. 2018, pp. 1,827-1,832, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6128063/>.
[43] Milad Iranshahy and Behjat Javadi, “Diet therapy for the treatment of Alzheimer’s disease in view of traditional Persian medicine: A review,” Iranian Journal of Basic Medical Sciences, vol. 22, no. 10, Oct. 2019, pp. 1,102-1,117, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6885391/>.
[45] See: Jamie Ehrenpreis, Carol DesLauriers, Patrick Lank, P. Keelan Armstrong, and Jerrold Leikin, “Nutmeg Poisonings: A Retrospective Review of 10-Years Experience from the Illinois Poison Center, 2001–2011,” J. Med. Toxicol., vol. 10, no. 2, Jun. 2014, pp. 148-151, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4057546/>.
[46] Note: Beside the fact that “[m]yristicin is present in nutmeg” – and the related “mace” – it’s also present in “…black pepper, parsley, celery, dill, and carrots.” This is according to the chapter titled “Toxins in Food: Naturally Occurring,” by D. Hwang and T. Chen, contributors to the academic volume Encyclopedia of Food and Health (Oxford and Waltham, Mass: Academic Press; Elsevier, 2016), edited by Benjamin Caballero, Paul Finglas, and Fidel Toldrá (text excerpted at <https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/myristicin>). However, I am reporting on myristicin in relation to nutmeg – and not in relation to other of the named plants – because the quantities are orders of magnitude higher in nutmeg, resulting in the fact that “…nutmeg and mace induce greater narcotic and psychotomimetic activity than” some other herbs, or even of “…an equivalent amount of myristicin or elemicin, also a component of nutmeg” separately. Ibid.
[48] Ehrenpreis, et al., op. cit. In fact, one report involved “…ten tablespoons of nutmeg.” Ibid.
[49] Eleesha Lockett, “Can You Get High on Nutmeg? Why This Isn’t a Good Idea,” Gerhard Whitworth, reviewer, Healthline, Aug. 31, 2018, <https://www.healthline.com/health/high-on-nutmeg>. Note that in a Google snippet, the article’s title displays as “High on Nutmeg: The Effects of Too Much and the Dangers”; whereas, on the actual Healthline website, the title reads “Can You Get High on Nutmeg? Why This Isn’t a Good Idea.” Presumably, the difference has to do with Search-Engine-Optimization (SEO) settings, which is an esoteric conversation that would implicate technical terms like “metadata” and “metatags,” and lies far afield from anything I’ll be delving into, presently.
[50] Of course, the focus of my work is on people with Alzheimer’s Disease and other forms of dementia. These conditions negatively affect memory and reasoning. Confused sufferers can sometimes expose themselves (or others) to dangers – whether advertently or inadvertently. For instance, one journal article reports on the case of one woman whose cognitively afflicted “…husband put nutmeg on his steak instead of pepper.” Els van Wijngaarden, et al., “Entangled in uncertainty: The experience of living with dementia from the perspective of family caregivers,” PLoS One (Public Library of Science), vol. 13, no. 6, Jun. 13, 2018, p. e0198034, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5999274/>.
[52] Niloufar Ansari and Fariba Khodagholi, “Natural Products as Promising Drug Candidates for the Treatment of Alzheimer’s Disease: Molecular Mechanism Aspect,” Current Neuropharmacology, vol. 11, no. 4, Jul. 2013, pp. 414-429, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3744904/>.
[53] Muhammad Ayaz, Abdul Sadiq, Muhammad Junaid, Farhat Ullah, Fazal Subhan, and Jawad Ahmed, “Neuroprotective and Anti-Aging Potentials of Essential Oils from Aromatic and Medicinal Plants,” Frontiers in Aging Neuroscience, vol. 9, May 30, 2017, p. 168, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5447774/>.
[54] “Researchers Call Herbs Rich Source of Healthy Antioxidants; Oregano Ranks Highest,” Science Daily, Jan. 8, 2002, <https://www.sciencedaily.com/releases/2002/01/020108075158.htm>; citing: American Chemical Society. On oregano outperforming other herbals in terms of its antioxidant abilities, see also: Snezana Agatonovic-Kustrin, Ella Kustrin, and David Morton, “Essential oils and functional herbs for healthy aging,” Neural Regeneration Research, vol. 14, no. 3, Mar. 2019, pp. 441-445, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6334595/>.
[55] Aleksandar Rašković, Isidora Milanović, Nebojša Pavlović, Tatjana Ćebović, Saša Vukmirović, and Momir Mikov, “Antioxidant activity of rosemary (Rosmarinus officinalis L.) essential oil and its hepatoprotective potential,” BMC Complementary and Alternative Medicines (alternatively titled BMC Complementary Medicine and Therapies), vol. 14, Jul. 7, 2014, p. 225, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4227022/>.
[56] As discussed in: Solomon Habtemariam, “The Therapeutic Potential of Rosemary (Rosmarinus officinalis) Diterpenes for Alzheimer’s Disease,” Evidence Based Complementary and Alternative Medicine, vol. 2016; Jan. 28, 2016, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4749867/>.
[59] Yan-Hua Lin, Ai-Hua Liu, Hong-Li Wu, Christel Westenbroek, Qian-Liu Song, He-Ming Yu, Gert Horst, and Xue-Jun Li, “Salvianolic acid B, an antioxidant from Salvia miltiorrhiza, prevents Abeta(25-35)-induced reduction in BPRP in PC12 cells,” Biochemical and Biophysical Research Communications, vol. 348, no. 2, Jul. 28, 2006 [online], Sept. 22, 2006 [print], pp. 593-609, <https://pubmed.ncbi.nlm.nih.gov/16890202/>.
[60] Mohsen Hamidpour, Rafie Hamidpour, Soheila Hamidpour, and Mina Shahlari, “Chemistry, Pharmacology, and Medicinal Property of Sage (Salvia) to Prevent and Cure Illnesses such as Obesity, Diabetes, Depression, Dementia, Lupus, Autism, Heart Disease, and Cancer,” Journal of Traditional and Complementary Medicine, vol. 4, no. 2, Apr.-Jun. 2014, pp. 82-88, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4003706/>.
[62] At least, it was the best among the five explicitly tested: bitter orange (Citrus aurantium), Fennel (Foeniculum vulgare), Mediterranean cypress (Cupressus sempervirens), Tasmanian blue gum (Eucalyptus globulus), and Thyme (Thymus vulgaris).
[63] Smail Aazza, Badiâ Lyoussi, and Maria Miguel, “Antioxidant and antiacetylcholinesterase activities of some commercial essential oils and their major compounds,” Molecules, vol. 16, no. 9, Sept. 7, 2011, pp. 7,672-7,690, <https://pubmed.ncbi.nlm.nih.gov/21900869/>.
[64] Yasiel Crespo, Luis Sánchez, Yudel Quintana, Andrea Cabrera, Abdel del Sol, and Dorys Mayanchaa, “Evaluation of the synergistic effects of antioxidant activity on mixtures of the essential oil from Apium graveolens L., Thymus vulgaris L. and Coriandrum sativum L. using simplex-lattice design,” Heliyon, Jun. 15, 2019, vol. 5, no. 6, p. e01942, <https://pubmed.ncbi.nlm.nih.gov/31245650/>.
[65] Soukaïna El-Guendouz, Smail Aazza, Susana Dandlen, Nessrine Majdoub, Badiaa Lyoussi, Sara Raposo, Maria Antunes, Vera Gomes, and Maria Miguel, “Antioxidant Activity of Thyme Waste Extract in O/W Emulsions,” Antioxidants (Basel, Switzerland), vol. 8, no. 8, Jul. 25, 2019[online], Aug. 2019 [print], pp. 243, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6719112/>.
[66] Masoumeh Asadbegi, Parichehreh Yaghmaei, Iraj Salehi, Alireza Komaki, Azadeh Ebrahim-Habibi, “Investigation of thymol effect on learning and memory impairment induced by intrahippocampal injection of amyloid beta peptide in high fat diet- fed rats,” Metabolic Brain Disorder, vol. 32, no. 3, Mar. 2, 2017 [online], Jun. 2017, [print], pp. 827-839, <https://pubmed.ncbi.nlm.nih.gov/28255862/>.
[67] Monika Sienkiewicz, Monika Łysakowska, Paweł Denys, and Edward Kowalczyk, “The antimicrobial activity of thyme essential oil against multidrug resistant clinical bacterial strains,” Microbial Drug Resistance, vol. 18, no. 2, Nov. 21, 2011 [online], Apr. 2012 [print], pp. 137-148, <https://pubmed.ncbi.nlm.nih.gov/22103288/>.
[68] Julie Jurenka, “Anti-inflammatory properties of curcumin, a major constituent of Curcuma longa: a review of preclinical and clinical research,” Alternative Medicine Review, vol. 14, no. 2, Jun. 2009, pp. 141-153, <https://pubmed.ncbi.nlm.nih.gov/19594223/>.
[72] Susan Hewlings and Douglas Kalman, “Curcumin: A Review of Its’ Effects on Human Health,” Foods, vol. 6, no. 10, Oct. 22, 2017, p. 92, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5664031/>. A similar extract is sometimes referred to as “bioperine.”
[73] Kayoko Miura, Hiroe Kikuzaki, and Nobuji Nakatani, “Antioxidant activity of chemical components from sage (Salvia officinalis L.) and thyme (Thymus vulgaris L.) measured by the oil stability index method,” J. Agric. Food Chem., vol. 50, no. 7, Mar. 27, 2002, pp. 1,845-1851, <https://pubmed.ncbi.nlm.nih.gov/11902922/>.
[74] Though, see my YouTube-video presentation Antioxidants, Part 2 to discover gamma-tocopherol, a form of Vitamin E more commonly found in seeds – such as sesame seeds, which are on my list.
[77] Also, pasteurization or processing can cause the vitamin content (especially in the case of Vitamin C) to diminish.
[78] Alexander Yashin, Yakov Yashin, Xiaoyan Xia, and Boris Nemzer, Antioxidants (Basel, Switzerland), vol. 6, no. 3, Sept. 15, 2017, p. 70, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5618098/>. Innumerable other articles could be given at this point, including many cited elsewhere in this post, or in any of the companion videos, but also: T. Alan Jiang, “Health Benefits of Culinary Herbs and Spices,” Journal of AOAC International, vol. 102, no. 2, Jan. 16, 2019 [online], Mar. 1, 2019 [print], pp. 395-411, <https://pubmed.ncbi.nlm.nih.gov/30651162/>.
In order to help pay for my dad’s nursing home care, my mom had to reduce her already modest assets as part of what is commonly referred to as a Medicaid spend-down.
But what is Medicaid? How do you qualify for it? Who is it designed to assist? And why do so many people have to expend their life savings in order to get it?
Let’s take a look at Medicaid.
In this introductory article, I’ll lay some basic groundwork – and provide a few essential definitions and concepts.
In two follow-up articles, we’ll discuss the all-important financial qualifications: first assets, then income. So… stay tuned!
(Also, be aware that this additional content is already available in the form of YouTube presentations and can be accessed HERE and HERE.)
Disclaimers
First of all, I need to give the usual disclaimers and in fact I want to amplify what I normally stay. I am not an attorney. I am not a financial advisor of any kind. You can consider the topics that I discuss to be research leads just to help you as you are thinking through these issues and hopefully help to shorten your learning curve in some of these important topics. But nothing that I say in this video should be construed as advice of any kind. If you need actual recommendations and evaluations, you need to consult with licensed professionals in your area. In this case, I am talking about attorneys who are knowledgeable about Medicaid, or other Medicaid experts.
The usual disclaimers are especially important in this case. That’s because Medicaid is just so complex; Medicaid’s rules and regulations are subject to amendment and modification; eligibility and other limits can be expected to change almost annually; Medicaid has as many different variations as there are US states.
So, you should meet with someone, not just is knowledgeable about the rough contours of the entire program, but somebody who knows the nitty-gritty of your local situation or state situation and how best to advise you.
What is Medicaid?
Medicaid is a United States government program that is designed to help impoverished people pay their medical expenses.
Sometimes, Medicaid is referred to as a joint federal and state program. Other times, Medicaid is referred to as a federal program that is administered by the U.S. states. And, sometimes, it is thought of mainly as a state program that has infusions of federal cash.
The federal government generally provides funding for benefits that are mandated at the federal level, which makes sense. The states, in turn, provide administrative services. They also pay for state-specific benefits.
However you think of it, or by whatever name you call it, Medicaid has a foot on the federal level government as well as on the state level.
This is one key reason for its (aforementioned) complexity. Namely, the particulars of how the plan is implemented and managed are going to vary according to the state that you are in.
Medicaid Isn’t Only for Long-Term Care
It is important to understand at the outset that Medicaid is a broad program and can cover many different medical services.
For example, it can cover routine doctor visits. It can cover hospital visits, long-term-care facilities, nursing homes and the like of that.
The long-term-care applications will be my focus in this series (since it’s the obvious concentration of the website). But Medicaid can cover a lot more than that.
And if you have need for additional services, for yourself or for your family, I am sure there are other resources that will expand my treatment.
Potential Pitfalls
Because of the complexity of the topic, there are certainly going to be a number of pitfalls.
Firstly, it’s easy to confuse Medicaid with Medicare. Not only are the two words similar, but both programs are overseen by the same government agency, the Centers for Medicare and Medicaid services, or CMS. CMS is a major division of the United States Executive Branch Department of Health and Human Services, with the cabinet-level Secretary of Health and Human Services at the helm of both programs.
However, these programs differ in terms of who is eligible and what services are covered.
Medicare is basically health insurance for seniors. Some of the premiums might vary in terms of the amount that is paid. But, otherwise, Medicare covers seniors of any income level.
Here, “senior” simply means a person who is 65 years of age or older.
There is an important caveat.
Medicare is called upon to deliver health coverage to people of any age, provided that they also are recipients of Social Security Disability Income (or SSDI), or if they suffer from end-stage renal failure (or kidney disease). Medicare itself is complex.
Medicare is a complex program itself. For my own YouTube-video treatment, see HERE.
In broad strokes, though, Medicare Parts A and B cover hospital and doctor visits, respectively. Part D was added to help provide prescription-drug coverage.
You can talk about something referred to as Medicare “Part C,” also known as “Medicare Advantage” plans. (These function something like Medicare HMOs)
And, to complicate matters further, Medicare Parts A, B and D can be further augmented with what are called “Medicare Supplement” (or “Medigap”) plans. (These, in turn, are also designated with letters like “Medicare-Supplement A,” “Medicare-Supplement F,” and so on.)
Medicare & Social Security
Historically, Medicare has a fairly tight relationship with Social Security.
For example, although it does have a deductible, Medicare Part A is usually delivered premium-free to people who are fully qualified to receive Social Security benefits. It is in this sense that Medicare Part A is often referred to as “automatic.”
It is important to note that if you are not eligible to receive Part A cost free, you may be able to purchase it.
Medicare has long had this close association with the Social-Security program
In fact, Medicare’s eligibility age, 65, once corresponded to the Full Retirement Age (or “FRA”)[1] for Social Security recipients. Even though the full-retirement age has been increased for most retirees, Medicare’s eligibility age has remained the same.
Medicare part B is never free. Though it’s actual premium cost will depend on many factors, including your income level.
Medicaid Will Be Our Focus
As stated from the outset, going forward, this series will be concerned with Medicaid (and its financial requirements), the government’s financial-assistance program for impoverished people – regardless of their age.
So, we come to one quick way of distinguishing Medicare and Medicaid.
Medicare has an age requirement,[2] but no income requirement. As long as you are 65 years of age, or older, you are eligible for Medicare.
On the other hand, Medicaid has no age requirement, but it does have an income requirement.
To rephrase: Medicare covers people 65+ years of age, of any income level; Medicaid covers any aged person, but only if they are of a low-income level.
Which Program Covers Long-Term-Care Costs?
“Medicaid also covers long-term care costs, both in a nursing home and at-home care. Medicare does not provide this coverage.”[3]
As noted by CNN, long-term care and nursing home costs are not generally covered by Medicare.
Medicare really only covers “curative,” skilled-nursing care – in a Medicare-approved facility. And, even then, it only covers skilled-nursing-home costs, provided that your entry into a qualifying facility followed a hospital stay of at least three days.
Additionally, Medicare coverage is calibrated to what are termed “episodes of care.” And each skilled-nursing-home visit is only covered up to 100 days per episode.
So, since Alzheimer’s and related dementias are not “episodic” in the relevant sense, we can basically say that Medicare is going to be irrelevant for the purposes of long-term care and nursing home care.
Another reason for this irrelevance is that long-term care is often bound up with what is called custodial care, and this is to be distinguished from skilled nursing care.
Basically, custodial care is help with the activities of daily living, whereas skilled nursing care is what you would normally think of in terms of medical care, medical testing, the administration of drugs, and the like.
(For my YouTube presentation explaining the difference between custodial and skilled nursing care, see HERE. For my written article on the same topic, see HERE.)
As if things weren’t confusing enough as it is, Medicaid is able to pay some of the expenses associated with Medicare. Examples of this would include the Parts B and D premiums, the Part-A premium (when it is applicable), and the various Medicare “co-pays” and deductibles.
Intro to Medicaid Eligibility
Each state sets its own guidelines for eligibility, within various limits.
For many states, Medicaid assistance is available to people who are below, at, or near the federal poverty level, or FPL.
Recipients cannot have incomes that exceed about 130-140% of the FPL, adjusted for household size. And these low-income requirements are very strict.
In addition, Medicaid recipients are not allowed to have much by way of assets or, in the Medicaid terminology, “resources.”
But, these two financial tests – one pertaining to assets, and one pertaining to income – are quite intricate. So much so, in fact, that I will be devoting a separate article to each of these.
So, I invite you to stay tuned for those posts.
And, in the meantime, feel free to view the companion YouTube videos. My discussion of Medicaid’s asset requirements can be found HERE, and my coverage of the relevant income requirements is HERE.
Notes:
[1] Note that, in some literature, this is instead termed the “Normal Retirement Age,” or NRA. Presumably, FRA is more common due to the fact that the letters “NRA” more commonly designate the National Rifle Association.
[2] For the exceptions to this, see the previous section.
A news item crossed my radar screen a couple weeks ago. This actually goes all the way back to August 2019, and was published in the Neurology, which is an academic journal, and subsequently was picked up by various news outlets.
I saw this through a press release from Washington University School of Medicine which is located in St. Louis, Missouri. The report focused on a new blood test that’s available for Alzheimer’s Disease.
Currently, it’s in testing phases. But, it has been developed, and researchers think that it holds great promise, and let me explain why that is.
So, first of all:
What does the test do?
I have both an ARTICLE and a YouTube VIDEO on some of the possible causes for Alzheimer’s disease. One of the causes that’s often referenced is the accumulation, in the brain, of various protein “gunk.”
There are two different types of protein that are implicated in this. The first is called beta-amyloid and the second is called tau. The two of these, together, account for the various “plaques and tangles” that Alzheimer’s patients’ brains seem to be riddled with.
The 100% definitive test for this is going to be an autopsy. (For these assortment of Alzheimer’s “tests,” see – again – either my other written work, e.g., HERE, or the companion, video presentation, HERE.)
There is very little use, obviously, for an autopsy to play in terms of preventative medicine or even in treatment, while somebody’s alive. It can give you the accurate cause of death only after the fact. But it’s not going to be too good for medicinal purposes.
Now comes a blood test that promises, or at leads holds the promise, of being able to detect levels of beta-amyloid in the blood during a person’s life.
Two kinds of beta-amyloid protein are being focused upon. And those are designated “Number 40” and “Number 42.”
My layman’s “take” on this is that there is an array of these beta-amyloid’s, but that 40 and 42 somehow play particularly important roles in the pathological accumulation of these deposits in an Alzheimer’s-afflicted brain.
I should say the test has actually been going on for couple years.
What researchers have hypothesized, and has since been borne out – at least, in early stages – is that levels of beta-amyloid in the blood suggest an accumulation of the beta-amyloid in the brain.
Why is the test important?
I mentioned that autopsies are the definitive test for Alzheimer’s. But, of course, autopsies are no good for diagnostic purposes so long as the patient is alive.
So, the most accurate test a living person can get right now is a so-called “Pet Scan,” which is shorthand for the more forbidding “positron-emission-tomography scan.”
A pet scan is essentially the best test that’s available.
But… pet scans are both expensive and time-consuming to perform. Therefore, this blood test holds out the hope for being able to be administered on a much wider scale and at far less of a cost.
Those are two points in its favor.
In theory, a blood test of this kind would be able to be given in a doctor’s office – instead of, for example, having to send the patient to an imaging center.
How Accurate Is the Blood Test?
What researchers discovered, when they compared the blood-test results against the pet-scan results, was that the blood test was 88% correlated with the pet scan.
What this seems to suggest is that, if for every 100 pet scans displaying evidence of Alzheimer’s, a blood test would detect Alzheimer’s in 88 of those cases.
At least… that’s the way I’m reading the article. (Disclaimer: I am not a medical professional! This is simply my untutored commentary on the situation. For advice, seek a healthcare expert who is familiar with your personal history.)
So, the test was (provisionally) determined to be 88% effective, in the above respect.
What Other Risk Factors Were Considered?
It’s worth pointing out that when they coupled the blood test with a couple of other risk factors – for example, age – the effectiveness increased.
It’s widely accepted that a person’s Alzheimer’s risk goes up with age. In fact, it’s said that your risk actually doubles every five years after age 65.[1]
Also, they factored in genetic predisposition. So, if you have the APO-E4 variant gene in your genetic makeup – as I myself do (see my video testimony, HERE) – then you have a higher (3 to 5 times higher actually!) chance of developing Alzheimer’s sometime in your life.[2]
Another risk factor – believe it or not – is sex. We talked about this in other places. (My AlzheimersProof.com post is HERE and my video is HERE.) Sex may not be its own risk factor. It may simply be that women live longer and therefore are more likely to manifest symptoms of Alzheimer’s and other dementias because of their longevity. But it is sometimes said that two out of three Alzheimer’s sufferers are female.[3]
When researchers incorporated age and genetic predisposition, they found that the test was 94% effective in terms of matching up to the pet scan.
What’s the Practical Benefit of an Alzheimer’s Blood Test?
But what they found, in addition to that, was that when some of the blood tests came up positive for people who had not yest been pet scanned, those people eventually came up positive on the pet scan as well.
This suggested to researchers that the test might actually be even more accurate than the pet scan, and able to detect Alzheimer’s in its very earliest stages.
Recall, also, that Alzheimer’s disease manifests in symptoms. But researchers believe that the underlying brain changes may take place as far back as a decade or more prior to the onset of symptoms.
One of the benefits obviously of early detection is they want to be able to treat people in presymptomatic stages. They feel like once memory changes, and other changes manifest in the brain, then that brain is already so damaged that it is basically beyond help.
In possibly being able to find people in the earliest stages of Alzheimer’s, another potential benefit of the blood test is that it might help with constructing clinical trials for developing interventions.
An early version of this test goes back to 2017 or even 2016. At that time, some of the articles referenced “autoimmune antibodies,” also called “autoantibodies.” The idea was that the immune system’s response to the accumulation of beta-amyloid protein might be able to be gauged. But, upon closer inspection of these articles now, in retrospect, they also seem to be describing a blood test that focuses on some of these beta-amyloid protein variants.
The fundamental idea is to try to catch Alzheimer’s disease in its very earliest stages.
Sometimes this “preclinical” stage is referred to variously as Very Mild Cognitive Impairment (especially on the so-called 7-Stage-Dementia view – about which, see HERE and HERE) or Mild Cognitive Impairment, often better known simply by the abbreviation “MCI.”
Note, however, that not all cases of MCI develop into Alzheimer’s disease. For one thing, there are other sorts of dementia (e.g., Lewy-Body Dementia, Multi-Infarct Dementia, Parkinson’s Disease, etc.) and there are traumatic brain injuries and other conditions that also might be prefaced by mild cognitive impairment. (For the difference between “Alzheimer’s Disease” and “dementia,” see my video, HERE.)
“Mild Cognitive Impairment” is, in a sense, just a catchall phrase for a certain level of mental diminishment as well as for the impoverishment of other perceptual and reasoning capabilities.
Concluding Reflection
There’s little doubt, though, that this blood test is fascinating. Even though it still has some way to go before you can expect it at a physician’s office near you, it holds promise.
Number one, it’s less expensive than the pet scan. Number two, it is able to be administered more widely, and in more environments – like doctors’ offices, and other places (such as out-patient clinics and “urgent-care” centers) – whereas the pet scan is obviously limited to an imaging center. Number three, it’s possibly more accurate than the pet scan. And, number four, it’s certainly superior to the autopsy in the sense that it holds out promise for being able to help treat and diagnose people while they are still alive – which is, quite obviously, advantageous.
People can end up in nursing-home and other long-term-care environments for any of several reasons. And residents may run the gamut in terms of their levels of awareness and disability.
When a resident retains his or her reason, then – in principle – he or she can “advocate” for themselves in the sense of communicating their desires and needs to facility administrators and staff. But what about cognitively impaired residents, such as those with Alzheimer’s Disease or some other form of dementia?
Such persons may require additional assistance. And this is where a Family Council can come in.
Long-Term-Care Resident Groups
Residents in long-term-care facilities, and families of people residing in such facilities, have the ability to form groups. These groups are often organized to facilitate discussions focused on resident needs and facility changes that may have to do with quality-of-care and quality-of-life issues.
As it happens, these groups, when formed, have tended to be referred to as “councils.” There are two main types of these councils that may be created: family councils and resident councils.
Resident Councils
The most basic variety of long-term-care group is going to be the resident council.
In general terms, a “resident council” is an association of individuals who live in a particular care facility and who wish to work together for the enhancement of their shared living experience.
When they exist, resident councils are independent of the care facility. To put it another way, the resident councils are not controlled or run by the facility administrators or staff.
I say that this sort of group is the “most basic” because it is natural for facility residents to provide feedback and input that pertains to their living conditions. They are interested in the facility, not simply in a psychological sense, but in an economic sense – that is, they have an interest in the policies and procedures of the relevant facility.
Family Councils
A related type of long-term-care group is the family council. As the name implies, “family councils” are groups organized and run by families (or close friends or representatives) of nursing home residents instead of the residents themselves. These family members then join with other families and speak for residents in advocating for policy and procedure changes that improve daily care and quality of life.
It should be said that nothing prevents residents from joining or participating in family councils.
Relatedly, I note that the point of the family council is not to compete with, replace, or supplant the resident council.
Rather, the point is to offer assistance to residents. And, the focus of this website being what it is – namely, Alzheimer’s Disease – it is important to observe that this assistance is especially necessary and valuable in cases where residents lack the ability to speak for themselves because of cognitive impairment, dementia, or similar conditions. (More on this, below.)
Brief Council-Related Questions and Answers (Q&A)
What Do Councils Do?
Both family and resident councils may bring to light issues surrounding care and living conditions. These may include, without limitation: the availability of food, medical equipment, silverware; the cleanliness of the facility; the functionality of things such as elevators; the reliability of internet access; and so on.
Essentially, any topic that impacts the quality of life of residents is fair game.
Once topics have been discussed, it is up to the individuals in the council as to how to proceed. Many facilities (see further on) are required to provide the council with a go-between or contact so that concerns can be delivered to the administration or staff without delay.
Councils may decide to bring their concerns to the facility orally or in writing – in a small group or via a designated council representative.
The first and preferable route would be to communicate with the facility.
However, if the facility is unreceptive for whatever reason, or if it somehow fails to satisfactorily address the expressed concerns, then councils may contemplate or undertake other actions.
Are Family Councils Only Allowed When Residents Have Dementia?
No. Family councils can be formed in order to support any person residing in a particular long-term-care facility, whether the resident is impaired or not.
However, it’s arguably even more important for a family council to be formed when resident loved ones do have cognitive impairments, since dementia sufferers may be unable to speak for themselves.
What Are Examples of Conditions That May Result in Cognitive Impairments?
What If a Resident Has No Living (Or Interested) Family Members?
Residents may give permission to non-family members to participate in family councils on their behalf.[1] If a resident has a cognitive impairment, then things can get a little dicey. If you would like a non-family member to represent your interests in a family council, you may wish to record your wishes in writings prior to the manifestation of any condition that might call in question your mental fitness.
Are Long-Term-Care Facilities (Such as Nursing Homes) Required to Recognize Family Councils?
I will address this question at greater length in a forthcoming post.
But, for now, suffice it to say that Federal regulation (in Title 42 CFR 483.10) states that Medicare/Medicaid-participating nursing homes must recognize family and resident groups when they form.
Further, these facilities have to provide resident and family groups with private meeting spaces, and they need to take reasonable steps (with the approval of the groups) to make residents and family members aware of upcoming meetings in a timely manner.
Additionally, the facility must provide a designated staff person to act as a liaison to the group. This person will be responsible for providing assistance to the group and with delivering (though not necessarily writing) responses to formal requests that result from the group meetings.
Does the Long-Term-Care Facility Have to Respond to Council Requests?
The facility cannot ignore the group or suppress its ability to form. So, in this sense, yes, the facility must provide some sort of reply to a group when it is asked to do so.
This does not mean, however, that the facility is compelled to do precisely what the council requests.
Things are tricky. I will try to explore some of these issues at greater length in a future installment.
Six Characteristics of a Family Council
It may be helpful if I briefly sketch some of the qualities that a family council will have.
Autonomy
Autonomy refers to the fact that the group is self-led. Neither a family council nor a resident council is created or led by facility administrators or staff members. If the facility has started and controls a group, then it is not a family or resident council in the relevant sense – regardless of what the facility calls it.
Facilities are of course free to form their own groups; and residents or families are free to join these facility-created groups if they choose to do so. But the formation of a facility-led group is not a replacement for an autonomous family council, and joining a facility group does not bar a person from joining an autonomous group.
Facility Specificity
There may be groups that support anyone living at any nursing home. However, a family council is relative to a specific facility. The ties that bind the members of a family council have to do with the fact that members all have relatives who live in the same long-term-care facility.
Independence
Independence is an extension of autonomy. The administration does not have claims over the family council. The councils are not dependent upon the facility. Moreover, the council is not considered to be a government program. It is an independent association of families of people living at a particular facility.
Interest
A family council must be made up of a group of people who have an interest in the facility. In this context, “interest” does not simply mean a curiosity. It means there has to be an interest in more of an economic sense. Member families have to have some “stake” in the facility and, going further, in the standards according to which the facility operates.
Openness/Inclusivity
There must be no barrier to entry into the family council other than having a close friend or relative involved in the facility. The council be must inclusive or open in terms of its membership.
Privacy
The group is owed a private space that should be provided by the administration of the facility on the facility grounds. The facility cannot appoint a staff member to “sit in” on the meetings.
Administrators or staff may be invited by the group to attend meetings. But, apart from such an invitation, presumably furnished by a council officer or spokesperson, the group should be allowed to meet privately.
Once again, the facility may endorse or sponsor other, staff-led groups. And these groups may also listen to complaints or solicit feedback from families and residents. But, the existence of such facility-controlled groups does not undermine the ability of residents and families to form their own councils to advance their own interests.
Notes:
[1] Presumably, if there is a conflict, a resident could also revoke a family member’s permissions or otherwise “block” one of his or her family members from participating in a council.
Within the United States and Canada there are laws that require a physician to report a patients with neurological or cognitive disorders to a licensing agency, as those patients may be a danger behind the wheel of a vehicle.
This type of reporting is not mandatory across the entire United States. Currently, there are only six (6) states that mandate a physician to report on a patient’s ability to operate a motor vehicle. These six states include:
California
Delaware
Nevada
New Jersey
Oregon
Pennsylvania
Not all mandatory states direct their reporting law toward those who are afflicted with Alzheimer’s Disease or, indeed, any sort of dementia whatsoever. Below are some specifics around each mandatory state and what is defined in their law.
If you want to see and hear me present the material, feel free to watch the YouTube video that I prepared, here:
California
The state of California is the first that I will discuss. It’s a prime example of a state in which (a.) there is mandatory reporting, and (b.) that reporting is at least partially concerned with Alzheimer’s Disease expressly.
The California Legislative Information website (leginfo.legislatures.ca.gov) references chapter 3 – Disorders Characterized by Lapses of Consciousness [103900-103990].
103900 states: “Every physician and surgeon shall report immediately to the local health officer in writing, the name, date of birth, and address of every patient at least 14 years of age or older whom the physician and surgeon has diagnosed as having a case of a disorder characterized by lapses of consciousness.”
This law specifically includes Alzheimer’s Disease as a disorder that involves the requisite “lapses of consciousness.”
In Delaware, the focus is on conditions that are characterized by “losses of consciousness.” In this respect, Delaware’s statutory language is similar to the “lapses of consciousness” verbiage present under California law.
Title 24 of the Delaware Code Online – Professions and Occupations Chapter 17, Medical Practice Act states: “Every physician attending or treating persons who are subject to losses of consciousness due to disease of the central nervous system shall report within 1 week to the Division of Motor Vehicles the names, ages and addresses of all such persons unless such person’s infirmity is under sufficient control to permit the person to operate a motor vehicle with safety to person and property.”
Again, for further reading, scroll down to “Delaware’s entry, HERE.
Nevada
Nevada is a good example of a state in which, while there is mandatory-physician reporting, it is not directed towards cognitive impairments such as dementia (of which, as we know, Alzheimer’s Disease is the most common variety). (On two ways of understanding the difference between Alzheimer’s Disease and dementia, see my YouTube video, HERE.)
According to the Bradley, Drendel & Jeanney law firm: “…Nevada laws can regulate the driving rights of individuals with epilepsy. In fact, doctors in our state are required to report epileptic seizures to the state’s Department of Motor Vehicles…”
You might be picking up on a recurring theme, here, but… for additional information, click down to “What does Nevada State Law say about Driving with Alzheimer’s?” in my 50-State Guide, HERE.
New Jersey
The New Jersey Academy of Ophthalmology, states, “NJ Law (N.J.S.A. 39:3-10.4) requires all physicians to report patients to the Motor Vehicle Commission within 24 hours after determining that a patient experiences any of the following: Recurrent convulsive seizures, recurrent period of unconsciousness or impairment, or loss of motor coordination due to conditions such as, but not limited to epilepsy in any of its forms which persist or recur despite medical treatment.”
Even so, New Jersey appears to be one of those states in which physicians could potentially be held liable, legally, if they don’t report potentially dangerous drivers.
While New Jersey law has established an elective reporting system for drivers with vision deficiencies and mandatory process for reporting specific neurological dysfunctions, there is no statute that protects a physician from liability if they have failed to report a patient that may cause injuries to a third party due to a condition known by the physician.
Given this, you might think that a New Jersey doctor will err on the side of reporting. And, I may be inclined to agree.
For more info, where do you think I’ll send you? My state guide, of course! Find it, HERE.
Oregon
The Oregon Driver & Motor Vehicle Services states: “Most medical professionals are required to report drivers who can no longer drive due to impairment.”
It is required of medical professionals to report on a patient’s impairment, even if that patient has agreed to give up driving.
The Oregon Secretary of State website similarly states: “…mandatory reporting by physicians and health care providers of those persons with severe and uncontrollable cognitive or functional impairments affecting a person’s ability to safely operate a motor vehicle.”
Cognitive impairments as specified in Oregon include: attention, judgement and problem solving, reaction time, planning and sequencing, impulsivity, visuospatial, memory and/or loss of consciousness or control.
Intuitively, this list is expansive enough to range over various cognitive impairments like dementia and Alzheimer’s Disease, even if they are not singled out for special or explicit attention.
See: “What does Oregon State Law say about Driving with Alzheimer’s?” which is a subsection of my longer, and more comprehensive (but certainly not exhaustive) reference, elsewhere on this website.
Pennsylvania
According to Schemery Zicolello Law Firm, the Pennsylvania Medical-Reporting Law requires health care personnel to report to the Pennsylvania Department of Transportation the full name, date of birth and address of every person over 15 years of age that is diagnosed as having a disorder or disability that could impair his/her ability to drive. In the list of reportable medical conditions, the attorneys specifically call out dementia.
That’s good enough for me.
If you want a bit more detail, scroll down to “Pennsylvania,” on my article, HERE.
Utah
Utah was mentioned in an article by National Center for Biotechnology Information (NCBI) as a reporting state. However, in the Fact Sheet for Patients and Families provided for Utah drivers, the indication for mandatory reporting by physicians is not present.
The document does state that the patient is expected to report and disclose their impairments to the department of motor vehicles.
So… I don’t find that Utah is actually a mandatory-reporting state.
Bear in mind that just because a state does not have mandatory-reporting laws, it should not be assumed that physicians won’t report anyway.
In the first place, a doctor might believe that it is his or her ethical duty to report a potentially dangerous driver – regardless of whether state law strictly requires that he or she do so.
Additionally, the physician’s other professional entanglements – for instance, his or her affiliation with a medical group or his or her professional-liability insurance – might have stricter requirements governing action steps in relevant cases.
Mandatory Medical Reporting Law States: In some states, physicians are required to report patients who have specific medical conditions (e.g., epilepsy, dementia) to their state Department of Motor Vehicles (DMV). These states generally provide specific guidelines and forms that can be obtained through the DMV.
Physician Reporting Law States: Other states require physicians to report ‘unsafe’ drivers to their state DMV, with varying guidelines for defining ‘unsafe.’ The physician may need to provide (a) the patient’s diagnosis and (b) any evidence of a functional impairment that can affect driving (e.g. Results of neurological testing) to prove that the patient is an unsafe driver.
Physician Liability States: Case law illustrates situations in which the physician was held liable for civil damages caused by his/her patient’s car crash when there was a clear failure to report an at-risk driver to the DMV prior to the incident.
On the NHTSA’s website, a survey of medical review practices can be found that indicate while all 51 jurisdictions accept reports of potentially unsafe drivers from physicians, only 6 jurisdictions require physicians to report drivers to the motor vehicle agency.
Another helpful article on NHTSA’s website is ‘Current Screening and Assessment Practices’. This article summarizes the legal requirements in each of the six mandatory reporting states.
Another helpful resource is the National Center for Biotechnology Information, the website for which can be found, here: https://www.ncbi.nlm.nih.gov.
National Library of Medicine, National Institutes of Health contains an article within the Journal of General Internal Medicine (abbreviated “J Gen Intern Med”). Of interest is an article titled “Reporting by Physicians of Impaired Drivers and Potentially Impaired Drivers,” which mentions that virtually all states have established policies for the identification of drivers with physical or mental impairments, however, the reporting is voluntary with the exception of specific states.[1]
Additional references on AlzheimersProof.com include:
This is a resource regarding the legalities of driving with Alzheimer’s or another cognitive disorder. This is not legal advice, simply research and research leads presented in a comprehensive article to assist in locating additional sources for further information. You can find additional information and important aspects specific to your state within my 50-State legal guide, HERE.
The above article, also on my website, goes into a discussion about a number of factors that may impact a person’s ability to drive, given their cognitive or mental state. This not only addresses that Alzheimer’s Disease occurs in stages (for more on which, see HERE), but also addresses some concerns around other cognitive impairments.
I also have an article – and a companion video (see my YouTube channel, HERE) – talking specifically about considerations of driving safety, apart from an explicit discussion on any legal requirements.
Now, if it gets to the point where you have to actually restrict your loved one’s access to the vehicle (and I sympathize with you if this happens), then you might find something of use in the above resource.
The final piece that I’ll note, here, is a general article that I did on the question of how to “Alzheimer’s Proof” a car. Recall that Alzheimer’s Proofing is akin, in this context, to baby proofing or childproofing. For more on this, see HERE.
Disclaimer
Please note – this article should not be treated as providing legal or medical advice, but purely as a reference that provides general information in regards to the laws that require a physician contact a licensing bureau in regards to a patient’s ability to operate a vehicle. This post is given as-is; I do not warrant that the information is accurate or complete. But I provide the information in good faith and I believe, to the best of my knowledge, that it is reliable.
Notes:
[1] As noted in the main text, the article’s list of states includes Utah, while in other references, Utah is not mentioned as a mandatory state.
Alzheimer’s Disease is a progressive, neuro-degenerative illness that presents itself in stages. While there is some debate over the precise number of stages (for more on which, see my ARTICLE or companion VIDEO), for present purposes, we can say that there are three: early, middle and late. Because cognitive degradation is just what it is to have some form of dementia, the fact is, at some point, an Alzheimer’s sufferer will become unsafe behind the wheel of a car.
In the early stage of Alzheimer’s, memory impairments may be mild affording a person the ability to safely drive. A larger concern occurs during the transition from the early to middle stage of the illness.
During the middle stage of Alzheimer’s, memory impairments may become more severe. You or your loved one may be doing fine one day, but have a lapse in memory or judgement, causing challenges the next day. These lapses, or deterioration in memory, can make a person with Alzheimer’s more of a danger to themselves or others, especially when driving.
By the time a person reaches the late stage of Alzheimer’s, he or she will have lost so many abilities (including language, mobility, responsiveness, etc.) that driving will be virtually inconceivable. Generally, by that time, the level of physical disability alone makes operating a motor vehicle practically impossible.
But before that threshold is reached, it may be somewhat difficult to identify the precise time at which a person becomes an unsafe (or at least unreliable) driver. Here is a breakdown of some early signs or symptoms that may indicate it is no longer safe for a person with this illness to operate a vehicle.
(These signs may be noticed by the person themselves, a loved one, vehicle caretaker or an outside party such as a neighbor, physician, police officer, etc. Additionally, it is important to assess behaviors and signs relative to a person’s “baseline.” In this context, a baseline is the starting point for comparison. It’s basically the way a person acted or the degree of functionality they possessed for most of their adult life – at a point when they were obviously not impaired in the relevant sense.[1])
Emotional Changes
A person with a mild demeanor may become more aggressive, hostile, or otherwise difficult. These changes in behavior could potentially be due to a mood disorder or other neurological problem. However, these behavioral changes can also occur in a person with Alzheimer’s Disease or some other form of dementia.
If you notice that you or a loved one becomes unable to control anger or depression, becoming so overcome with emotional fits or episodes, it may be an indicator of Alzheimer’s or some other serious condition. Whatever the cause, these emotional changes will increase the dangers and risks of being behind the wheel of a car.
Anger – Your loved one may become agitated or irate with little or no apparent provocation, or beyond what a normally functioning person would think of as justified or reasonable.
Anticipation – In this case, the pathological component may be another outgrowth of memory loss. If you loved one seems or professes to expect or hope for an imagined or past event, it may be a sign of worsening dementia.
Disgust – An Alzheimer’s patient may have difficulty masking emotions and might display naked aversion, distaste, loathing, revulsion, etc. even in inappropriate contexts or directed toward things that they previously felt fondly toward.
Fear – On a low level, this might result in an increasing level of anxiety. It could be apparent through spoken language, but it may only become apparent to people who notice subtler signs or body language (e.g., in facial expression or posture) or habit (such as hand wringing or nail biting). Alternatively, fear may manifest in more extreme ways, for instance, through indications of a pathologically paranoid or suspicious turn of mind.
Joy – We all like to see our loved ones content and happy. But, in some cases, the level of jubilation or excitement may exceed what is appropriate to or warranted for the occasion. For instance, your loved one may not exercise due restraint. Alternatively, it may appear strike you as inappropriate in the sense that he or she seems to be taking pleasure in something that ought to elicit a different emotional reaction.
Sadness – A dementia-afflicted people might suffer from apathy or depression, or from some other related sort of unrelenting melancholy. They may tend to brood or become removed or withdrawn from family or other social circles.
Surprise – Look for evidence or amazement or bewilderment that seem out of place. Astonishment or shock could be a result of affected judgment or reasoning. But it also could be a function of increasing forgetfulness and impaired memory.
Trust – This may be related to fear and paranoia in the sense that your loved one may begin to suspect family members of plotting against them. Contrariwise, it might be expressed in an inappropriate or unwise willingness to follow or receive instructions from strangers.
Memory Changes
Some Alzheimer’s-afflicted individuals may have issues with short-term memory loss but are able to remember things that occurred further back in time. Vehicle operations can be broken up into “before,” “during” and “after” categories to determine if memory changes impact or undercut safe driving. Here’s what I mean.
Before Getting Into the Vehicle, Ask…
Do you or your loved one have an issue finding the keys?
Is it consistently a challenge to remember where the vehicle is parked? Or…
Is it hard to recall which vehicle belongs to you?
Everyone misplaces things from time to time. Obviously, when it is sporadic, this is not necessarily an indicator of Alzheimer’s Disease or some other form of cognitive impairment or dementia. However, the issue occurs when this becomes more of a pathological condition where memory loss is more frequent than normal, or when its occurrence undermines safety.
While Inside of the Vehicle, Ask…
Do you or your loved one have trouble remembering which pedal is the accelerator and which is the brake?
Is there confusion on what traffic signs or signals are indicating?
Do you or your loved one regularly forget where you are going, or how to get there?
Beyond the perceptual diminishment that often accompanies normal aging, cognitive impairments may erode sensory faculties. Does the driver have reduced sensory-processing capabilities? (See further below.)
Do the A/C or radio controls confuse you or distract you from the road?
A person with this illness may not understand signs to where they inadvertently drive through a construction zone. They may also forget where they are going or how to get where they are going, even if the route is familiar.
After Exiting the Vehicle, Ask…
Are there dents or scratches that cannot be accounted for?
Is parking haphazard or erratic?
Are items forgotten inside the car inadvertently?
Are keys routinely left in the vehicle?
Is the car left running unintentionally?
Have you or your loved one begun to receive mailed traffic citations? Or…
Is the driver being pulled over more frequently than before?
A person afflicted with this some form of dementia or other cognitive difficulty may not remember how a particular dent or scrape appeared on the vehicle.
All these items are warning signs or indicators that something else may be going on beyond normal forgetfulness.
Motor-Skill Changes
Cognitive disabilities are only half of the picture, though. Driving also places physical demands on a person. Therefore, various physical impairments can also undermine safe-driving abilities.
Similarly to the previous category, these changes can also be evaluated by looking at requirements that impose themselves before, during, and after using a vehicle.
Before Getting Into the Vehicle, for Example…
Changes in motor skills or reductions in physical strength may hinder a person from doing something as simple as opening or closing a vehicle door.
You or your love done may struggle with opening or closing the hatch or trunk.
It may become difficult or practically impossible properly open or close the hood of a vehicle.
It is true that memory may come into play here as well. And there’s little question but that forgetting how to do these minor tasks may be an indicator of Alzheimer’s.
But diminished motor skills can be serious problems on their own. And, when determining a person’s driving fitness, physical abilities need to be assessed alongside cognitive ones.
While Inside of the Vehicle, for Example…
A person with diminished motor abilities may have difficulty turning the wheel.
He or she may have trouble physically depressing the pedals or shifting gears.
Someone might find it physically taxing to keep the car in the correct lane.
Parking the vehicle may begin challenging, especially if the individual has limited abilities to turn their body or head.
Sensory impairments such as hearing or vision loss can also undercut the ability to safely operate a car or truck.
After Exiting the Vehicle, for Example…
Do you or your loved one have difficulties just physically getting in and out of the house, opening entry or garage doors, carrying groceries, and so on?
Of course, people often drive in order to assist them with the functional activities of life – such as shopping. While general impairments may not specifically speak to the question of safety behind the wheel, they do speak to the issue of whether driving is beneficial or necessary. If you or your loved one can no longer perform or engage in other life activities – like shopping – then it may be that driving is no longer helpful. This suggests that it may pose a risk that outweighs any potential benefit.
Additionally, the loss of non-driving-specific abilities indicates a general physical decline any may suggest either that driving-related abilities may soon erode or that further cognitive impairment is on the horizon.[2]
Clearly, being unable to physically control a vehicle, while not an Alzheimer’s-specific problem, may be an indicator that you or your loved one can no longer reliably or safely operate a vehicle.
Perceptual Difficulties
The normal aging process can cause perceptual difficulties. However, Alzheimer’s can exacerbate these issues.
Perceptual difficulties may impact visual-spatial abilities such as being able to judge distance or peripheral vision. Being spooked by shadows or not noticing cars or pedestrians next to you may be a result of diminished perception.
There may also be an inability to see traffic signs, signals, or other drivers (for example, people braking in front of them or merging into the same lane).
Perceptual difficulties may also include a decreasing ability to hear sirens or horns. This poses an obvious danger – especially, though not exclusively, if it is coupled with memory impairments. Forgetting what emergency-vehicle sounds indicate or require in terms of courses of action can lead to accident, injury, or death.
Reasoning Changes
A deviation from a normal route may cause confusion for a person with Alzheimer’s, as they may not be able to react or think through an alternate route. They may also have issues navigating around accidents or construction sites.
A person with this disease, or some other form of cognitive impairment or dementia, may have a reduced reaction time that, in turn, undermines their ability to react to unexpected changes within their route. These include such things as closed roads and bridges, etc., which could potentially lead to accident, and certainly engender confusion.
Deviations and detours can also result in you or your loved one becoming lost.
Concluding Remarks
As difficult as this can be for the afflicted individual, there will come a point where having them behind the wheel of a car or truck will become more of a danger than a benefit.
For more information, please see my companion YouTube video, HERE.
Postscript
In addition to these safety considerations, there may also be legal implications and potential liabilities in regards to a person driving with Alzheimer’s Disease.
While I am not a lawyer or legal expert, I do have several, relevant resources available on AlzheimersProof.com.
[1] Of course, some persons may have lifelong afflictions or disabilities. These will have to be factored in as well. Doing so is beyond the scope of this article. Consult a healthcare or medical professional for personal evaluations or recommendations.
One of the major challenges in caring for someone who has Alzheimer’s Disease, or some other form of dementia, is that they are often prone to “elopement.” Of course, in the context of long-term care, elopement has nothing to do with illicit or surreptitious marriage. It has to do with a cognitively impaired person leaving the safety of the care environment without supervision.
This problem can be extremely vexing for the caregiver and perilous for the Alzheimer’s sufferer. I know this firsthand. On one memorable occasion, my dad was returned to his home by a police officer after he had been found wandering along a busy road in our city. During a snowstorm.
However, I was able to hinder my dad from wandering with an ingenious little gadget. In this article, I’m going to explain how to install that device – a door blocker called the “Defender.”[1] I have installed several of these blockers: one in an apartment, and a couple of them in a townhouse. I absolutely love these products. And I think that you might, too.
Introduction
What’s the Function of the ‘Defender’?
Knowing your loved one can open doors and leave the care environment without you or a caretaker in tow – or even realizing your charge is gone – is a terrifying proposition. Memory and reasoning deficits raise the possibility that he or she could become disoriented and lost, or even injured or worse.
From the perspective of long-term home care, then, the main benefit of these locks is to prevent your loved one from eloping. The devices are inexpensive, and the contemplated modification may be performed relatively easily.
This sort of change is part of what I mean by “Alzheimer’s proofing” your home environment. (This is a concept that I describe more fully HERE.) Under this way of using the phrase, it is a close cousin to childproofing a house as expectant parents would do in preparation for the arrival of a newborn.
Devices Double as Theft Deterrents
These door blockers can deter Alzheimer’s sufferers, or other cognitively disabled persons, from opening exit doors, leaving the care environment, and potentially putting themselves in harm’s way.
But it is worth noting that this particular use – keeping someone inside the house – is a bit of a departure from the product’s stated purpose.
This style of door lock has been designed and marketed as a security device and theft deterrent. When properly installed on an entrance door, the lock helps to prevent forcible entry into a house. It essentially fortifies the door so that even if a thief has jimmied it, or defeated its deadbolt and locking mechanisms, the door blocker will enable the door to remain in a closed position.
So, beyond the standpoint of Alzheimer’s proofing, it will add another layer of security to your home.
Can Your Alzheimer’s-Afflicted Loved One Defeat the Blocker?
As stated, the Defender is intended to be set into a locked position inside the home in order to reduce the probability of forcible entry should an intruder attempt to gain access to the interior of your house.
Given this, it has been designed to be locked and unlocked by normal-functioning adults. Therefore, it is possible for a cognitively impaired person to operate the latch. However, to do so he or she would have to have a number of cognitive and physical abilities. A rough-and-ready enumeration of these might look the following.
Cognitive Abilities Plausibly Needed to Defeat the Blocker:
The ability to notice the device
The capability to identify its function
The capacity to understand or the resourcefulness to determine the correct way to unlock it once
The motor skill and dexterity required to execute the unlocking action
The memory power to remember how to defeat it on subsequent encounters
I’m certainly no medical or psychological expert. But, the likelihood that a cognitively impaired individual would possess this collection of abilities seems to me to be somewhat low. More guardedly, I suppose that I would venture the opinion that the probability is low at least once your loved is sufficiently advanced in his or her dementia to be a serious elopement risk.
Often, if it is positioned high enough on the door – or if it is camouflaged – your loved one may not even recognize that the door blocker has been installed. Of course, this is because Alzheimer’s tends to diminish perception. In the case of my dad, for instance, I don’t believe he noticed that the thing was even there.
Additionally, a high-up position might hinder the door-opening ability of a senior adult in general – quite apart from any dementia – for example if he or she has joint or mobility issues.
Moreover, the door blocker requires an additional motion, outside of those used to open doors in the usual way, that may frustrate a person with a cognitive deficit and prevent them from eloping from the home.
WARNING!
I should, however, inject an important word of caution.
These door blockers may hinder your and your loved one’s abilities to exit the house in the event of a fire or other emergency. If you’re going to use these products as a deterrent to help prevent elopement of a loved one from the residence, you may want to ensure the blocker is activated only during the time periods where your loved one is at the highest risk of vacating the premises without you noticing.
Of course, from a theft-deterrence perspective, it is appealing to have the latch activated throughout the night or during whatever intervals occupants of the house wish to lower the likelihood of intrusion.[2]
Disclaimer:
I cannot advise you as to the appropriateness of any particular course of action for your application. Furthermore, I cannot be sure, and do not warrant, that the device will be effective for you – for any purpose whatsoever. This information is presented as-is, for general or entertainment purposes only. Whatever use you put this information to is entirely your own responsibility. No one at or affiliated or associated with AlzheimersProof.com assumes any liability for how you may implement or not implement any of the ideas described in on this website or in any companion videos.
Be aware of where and under what circumstances you are installing these blockers. The upshot is that I am certainly not guaranteeing that these devices or installation methods will be successful or safe for your individual or family situation.
I can only state that these blockers were a tremendous help for me and my family when caring for my Alzheimer’s-afflicted dad.
My Installation Procedure
‘Unboxing’ & Collecting Required Tools
‘Defender’ Installation Instructions
Upon opening the Defender’s packaging, you will find several items. These include:
The door blocker device itself;
Instructions;
3 large wood screws;
4 smaller metal screws;
Tools
The main tools needed include:
A drill (this could be theoretically be corded or cordless; mine was the latter)
1/8-inch drill bit
Philip’s screwdriver
Optional (& Possibly Necessary) Tools
Wood chisel (if there is insufficient space in between the door and door jamb to accommodate the blocker)
Hammer (to use the chisel, if one is needed)
Center Punch (to tap a small “pilot” for the drill bit)
Tape Measure (to assist in positioning the blocker on the door with respect to the other locking hardware – such as doorknobs and deadbolts)
Safety Equipment
Safety goggles
Positioning the Blocker
You may want to begin by determining where you want to place the Defender door blocker. The instructions suggest that it be installed at least 6 inches above the door handle and deadbolt.
As suggested above, it may be beneficial to install this blocker a bit higher than this. In fact, there is an “L-shaped” area on the door within which the manufacturer recommends placing the Defender.
Inverted ‘L’-Shaped Install Location
While determining where to install the blocker, place the blocker in the locked position. While in this fully closed position, slide the plate between the door frame and door with the black pad against the door.
This will allow you to get a good look at everything, and to reposition the blocker is desired or necessary.
**Be mindful of any electrical outlets nearby as there may be wiring within the walls near where you may be drilling. Additionally, look at surrounding door hardware, molding, key hooks, or other things that might interfere with your ability to operate the blocker and allow it to swing fully from locked to unlocked positions, and back again.
Actual Installation Steps
Step One
Once you have determined where you want to place the door blocker, use a pencil to mark the placement of the center screw within the door frame.
Step Two
Use your drill and 1/8-inch drill bit to make a hole where the center screw will be placed.
Step Three
Place the door blocker plate back against the door frame, allowing the recently drilled hole drilled to be visible in the center-hole of the plate.
Step Four
Drive the center screw into the door frame allowing the blocker plate to be provisionally positioned. The center hole is oval shaped and allows for the back-and-forth movement of the device in order to ensure that it is tight enough against the door to perform its function, but not so tight that it prevents you from latching and unlatching it.
Step Five
Test for the appropriate and desired fit. Before fully securing the door blocker, close the door and test the blocker in the locked position to ensure the placement is optimal. If the lock is difficult to engage or disengage, the placement of the plate may need to be adjusted slightly for proper operation of the device. In this case, you would simply loosen (but not remove) the center screw, move the blocker, and re-tighten the screw.
Step Six
Once the positioning has been established, ensure that the center screw is fully tightened – but not over-torqued. (You don’t want to strip the head or threads.)
Longer Wood Screws & Shorter Metal Screws
Then, drive in the remaining three (3) screws – large screws for a wooden door frame; small screws for metal – into the remaining holes present on the door blocker plate to firmly secure the blocker.
Congratulations!
Your Defender door blocker has now been successfully installed!
‘Defender’ in Position
If you need an additional assist, or a bit more in the way of visual aids, never fear. For a demonstration of the operation of the lock, or for a video tutorial on the installation procedure, please view my companion YouTube video: Alzheimer’s Elopement & Access Control: Install the Defender Door Lock.
Thank you for reading! I wish you all the best trying to deal with elopement risk.
Notes:
[1] The “Defender” appears to me to be an off-brand version of a different door blocker known as the “Door Guardian.” I also have the Door Guardian and will walk through its – nearly identical – installation procedure in a subsequent post.
[2] Note that there is no “key” and that the device is not designed to be unlocked from the outside. It is supposed to be activated and deactivated from within the area being secured.
“Custodial care” is nonmedicalhelp with the Activities of Daily Living (like bathing and eating). “Skilled care” is medical care, such as giving medications and shots, dressing wounds, drawing blood, and so on.
The phrase “long-term care” can be confusing, since custodial care is sometimes used as a synonym for custodial care, and sometimes it’s used for the combination of custodial and skilled care that a person might receive in a nursing home.
I would like to spell these things out as simply as I can.
So, let’s first think, on a very basic level, about what we mean by long-term care.
A Personal Example: My Dad
As I have written elsewhere, my dad, Jim, passed from Alzheimer’s disease in 2016. I took care of him in his own home for four years. And then he was in a nursing home for four years after that.
That means that he suffered obviously from Alzheimer’s for at least eight years. In fact, it was longer. We can reasonably conclude this for two reasons.
Firstly, I started caring for him was because it was becoming increasingly apparent that he needed help. So, we are justified in believing that he was suffering from some cognitive impairment before I assumed the role of his daytime caregiver.
Secondly, scientists inform us that the brain degeneration of Alzheimer’s begins before any symptoms manifest themselves. Therefore, we can infer that Jim had the very beginnings of Alzheimer’s prior to anyone noticing that something was wrong with him.
But, once we became aware, we observed that he needed help with the basic tasks of everyday life.
Help With Everyday Activities
Called “Activities of Daily Living,” or “ADLs,” these include things like bathing, dressing, eating, maintaining continence, toileting by yourself, and transferring in and out of bed.
These are things we all need to do each day. That’s 24/7/365, as it were.
That’s the intuitive definition of “long-term care.” It’s help with the ADLs, delivered over a fairly long period of time.
So, what’s in view here is a person who has a chronic condition, disease, disability, or whatever and who is going to require everyday care over a long period of time.
Probably Also Need Extended Medical Care
It turns out that many conditions that will prompt this level of care are also terminal conditions. (I go into greater depth on terminal illnesses HERE and HERE. And I have a video on the topic, HERE.)
A personal who is so severely incapacitated that he or she needs daily assistance with the basic activities of living most likely also requires some kind of ongoing medical care.
Think about my dad, again. He had Alzheimer’s Disease. He required both medical care and nonmedical care. He needed supervision and medication, for instance.
As noted previously, one way of using the term “custodial care” is applying it to nonmedical care. But, a person – like my dad – who has a chronic and debilitating illness may very well also require medical care (e.g., pharmaceutical interventions, speech therapies, and so on). When we say “skilled care,” then, we’re thinking of this latter sort of care.
Possible Word Confusion: ‘Long-Term Care’
Once again, the intuitive difference between custodial care and skilled care is going to be that custodial care is essentially nonmedical / supervisory care, whereas skilled care is going to be medical.
Now there are a few different ways of kind of getting more clear on what the differences are, and I’m going to talk about what the actual care is in terms of (1) what is involved, (2) who provides the care, (3) where the care is provided, and (4) how you pay for it.
But before I do that, let me just say one another word about long-term care.
Sometimes, often in everyday speech, the word “long-term care” is used to encompass both custodial and skilled care. In this loose sense, long-term care basically means “whatever your loved needs over an extended period of time.”
A person may think about a relative who’s in a nursing home – like my dad was. My dad received both types of care in the nursing home. So, it’s tempting to think that my dad’s long-term care had medical and nonmedical elements. He needed both – over the long term.
Other times, the word “long-term care” is essentially used as a synonym for custodial care. This use is common in billing applications, healthcare insurance, long-term-care insurance, Medicare, Medicaid, etc.
The upshot is: understand the context of the word use. And, when you hear it, be sure that you know which definition of the word is operative!
‘Qualifying’ for Long-Term Care
What I mean, here, is essentially this: What are the diagnostic triggers that would prompt a doctor to say, “This person needs long-term care”?
This is an important consideration, especially – but not exclusively – for people who may have private nursing-home and other pertinent insurance policies. Long-term-care insurance generally “kick in” once the insured person is certified as being in need of long-term care.
2 Triggers
Physical
This is measured in terms of the “Activities of Daily Living,” or ADLs. In most materials, you’ll find six of these listed. I mentioned them, above: Bathing, dressing, eating, transferring, toileting, and controlling bodily functions.
From the physical point of view, to be “long-term-care certified” essentially means that you lack two out of six of these activities. So, if you’re incontinent and unable to feed yourself, then that would count. Or, if you’re unable to dress yourself and get in and out of bed by yourself, that would count also.
Your needs will have to be evaluated and documented by a licensed healthcare professional, chiefly, a physician.
Cognitive
But there’s also a cognitive or mental trigger.
You may also be certified as in need of long-term care if you have a cognitive impairment to a significant enough degree that you would require more or less constant supervision in order not to hurt yourself or other people.
Sometimes this trigger is pulled at the same time as the physical one, and other times the two are quite separate. In my dad’s case, for instance, he was physically able-bodied (in terms of the ADLs). He had no physical difficulties.
His problem, initially, was purely cognitive. Of course, as the disease progressed, his condition worsened and then he met the long-term-care qualification “tests” multiple times over. This is not uncommon.
Lacking Activities of Daily Living = Custodial Care
When you think of these Activities of Daily Living – bathing by yourself, dressing, feeding, and so on – think custodial care. Likewise, think of custodial care when you think about severe cognitive impairment that necessitates supervision.
Custodial care is going to be that kind of care that assists a person in receiving and in performing the Activities of Daily Living or providing the needed supervision.
Medicines, Medical Tests, Therapies, Etc. = Skilled Care
But my dad’s Alzheimer’s Disease also required certain pharmaceutical interventions. He was on put on the drug Aricept, for example. And it had to be administered to him at various times.
Of course, family members are able to administer that kind of medication at home. But in an institutional care situation, you wouldn’t want a person who doesn’t have proper licensing and proper credentials to administer drugs to your loved one.
But, as of this writing, people don’t need to be licensed to help bathe your loved one, or to help feed him or her.
Therefore, a second distinguishing feature of custodial care is that the care practitioners do not need to be licensed.
On the other hand, skilled care, as the medical portion of care, does require special training and licensing. In fact, that is one of the reasons it is referred to as skilled care.
Nursing Homes Provide Custodial & Skilled Care
In certain care environments, you are going to see a combination of these needs being met. So, for instance, a nursing home is a place that is going to provide both custodial and medical care for its residents. It’s a one-stop shop, so to speak.
One of the reasons why these definitions get a bit mixed up is because of the fact that we see our loved ones in this kind of composite care environment. It’s therefore natural to assume that everything going on in that environment is appropriately called “long-term care.”
Possible Care Environments
Of course, other care environments exist beside the nursing home.
Home Care
Number one, a person could receive care in his or her own home, or in the home of a friend or relative. Certainly, you can have people come into the home to provide the kinds of custodial supports that a person might need. And, generally speaking, if you’re receiving care in the home the professional care is probably going to be a supplement to a familial caregiver.
When my dad was living in the home, it was my mom and who were giving the supports that were necessary for him to get through the day. But, if we needed additional help, then we might call somebody else to the house.
This extra support could be skilled – like a visiting nursing – or unskilled/custodial. But, for the most part, we handled the custodial portion of the care ourselves.
Assisted Living
An assisted-living facility is a place that’s going to help people who are starting to have difficulty with the Activities of Daily Living. Such facilities try to emphasize and encourage independence. Seen from a different perspective, these facilities actually require a fair degree of independence – since they are generally not licensed or staffed to provide the level of care available in nursing homes.[1]
Nursing Home
But, for present purposes, the third main care environment is a nursing home.[2]
A nursing home is going to provide a level of care that’s a notch above an assisted-living facility in terms of comprehensiveness.
Whereas an assisted-living facility is equipped to provide low-level help with some daily activities, a nursing home is able to provide full-blown custodial care.
And whereas an assisted-living facility likely has a nurse or doctor on call, a nursing home always has medical practitioners on the premises. Skilled care is part of the overall care provided by the home.
To put it slightly differently, nursing homes provide comprehensive care services.
Billing of Services
Why are these distinctions so important?
Well, the distinctions become important largely when it comes time to pay the bill!
As usual, this discussion can become nuanced and detailed. But here’s the bottom line.
There are three main ways to pay for long-term care services, broadly construed.
Private Pay
“Private paying” is where you pay for yourself. You’ll likely do this out of your own assets (e.g., checking, money market, savings accounts; emergency funds; retirement vehicles; etc.) or your own income (for instance, annuities, pensions, rental payments, social security, and so on).
While you pay for yourself, you can go wherever you can afford. You can have whatever accommodations and services you like. At least, you can have all this so long as your money holds out.
At the level of nursing-home care, your bill is likely going to be a composite of skilled nursing services and custodial services. But if you’re paying entirely out of pocket for your care, then it doesn’t matter which sort you’re being billed for. You pay for everything yourself, regardless of what type of care it is.
So, in the private-pay scenario, the custodial/skilled distinction really doesn’t matter from the standpoint of your checkbook.
Government Aid
Medicaid
Once you “spend down” your assets to a particular – and low – level, you may be eligible for Medicaid. This is a government-assistance program that is geared towards helping impoverished people pay for necessary medical expenses.
For qualifying individuals, Medicaid pays for (portions of) both custodial and skilled care. However, there are strict asset and income tests that are applied.
Moreover, your preferred facility may not be able to accommodate you. Some facilities have no or few “Medicaid beds.” Others require that you have lived at the facility under private-pay arrangements for a specified period (not infrequently one or more years) before you can claim a Medicaid bed. Others have long waiting lists.
Typically, the relevant beds are in semi-private rooms with at least one other occupant. Additionally, Medicaid usually segregates its recipients by sex.
Medicare
What about Medicare?
For purposes of this post, let’s just say that Medicare is a government program that provides healthcare coverage for seniors (i.e., people over the age of 65).
In principal, then, Medicare is available to cover at least some of the medical-related, skilled-care portion of the nursing-home bill. Now, there are several caveats.
One of these is that Medicare only really covers hospital bills and short-term skilled-nursing costs.
Additionally, there are requirements that the skilled nursing, to be covered, must follow a hospital stay.[3]
Curative Vs. Palliative Care
Finally, Medicare is geared toward what is called “curative care.” In basic terms, this sort of care is supposed to (help to) restore a person back to good health.
“Palliative care,” on the other hand, merely relieves symptoms – it doesn’t “cure” a patient.
You run headlong into trouble, here, when you start to consider conditions, like Alzheimer’s Disease, that have no cures.[4]
Elsewhere, I have discussed the question of whether Alzheimer’s is a “terminal illness.” (For a written article, see HERE. For a video touching the issue, see HERE.)
But suffice it to say that Medicare doesn’t generally cover palliative care – except in end-of-life, hospice situations.
The Upshot
The long and short of it is this, then.
Medicare only covers short-term skilled care and curative care.
Custodial and palliative care is generally not covered by Medicare at all.
Medicaid may cover these – is a person is eligible based on asset and income qualifications.
But that means that if a person is receiving both custodial and skilled care in a nursing home, and even if Medicare is paying for some of the medical/skilled portion of their bill, they cannot rely on Medicare to pay for any of the help they get with Activities of Daily Living. And they cannot hope to get Medicaid assistance until their own assets are spent down.
Long-Term-Care Insurance
Besides paying out of your own assets and spending your own assets down until you qualify for Medicaid, really the only other payment option is to use proceeds from a long-term-care insurance policy.
Such policies have a high application-decline rate, partly because people generally wait so long to try to purchase them.
Now I get more in depth into long-term care in other places. But, essentially, long-term-care insurance is the kind of insurance that’s going to help you to pay for the nonmedical portion of your bill. Long-term-care policies pay benefits when you need custodial care.
So, if you are getting help getting paying for the medical or skilled-care portion of your bill via your health insurance or via Medicare, then a long-term care insurance policy is able to pay for the custodial-care portion.
Of course, you have to be long-term-care eligible in order to collect payouts from this type of policy.
Basically, “eligibility” comes to this. You have to lack two of six of the aforementioned Activities of Daily Living, or you have to be cognitively impaired to such an extent that you require supervision.
But, once a physician “certifies” you as long-term-care eligible in one or both of these ways, then your long-term-care policy is supposed to pay out.
Only a few policies these days have lifetime benefits. So, you should be aware that is it possible to exhaust the proceeds of such a policy. But, it does constitute a third possible funding option, and can delay or avoid exhaustion of your personal assets.
Confusions Summarized
One confusion arises with respect to the fact that “long-term care” is a phrase that can be used for both types of care, together, or as a strict synonym for custodial care only.
A second confusion comes from the fact that both kinds of care – custodial and skilled – are delivered side-by-side, in the same environments. For example, and as discussed, you may get both medical and non-medical care in a nursing home.
Thirdly, there are confusions with respect to how care is billed. What you have to realize is that nursing-home bill is going to be a conglomeration of items, some of which are going to count as custodial services, and others of which are going to be skilled. Who pays – and what kind of insurance or assistance is relevant (e.g., health or long-term-care insurance, Medicare, or Medicaid) – is going to depend in part on this classification.
The Major Issue Restated
For most people, the main point of learning the distinction between custodial and skilled care is to gain clarify and insight into the question of how the relevant types of services can be paid for.
Who pays for a particular care service and for how long is, in part, a function of whether the service is classified as “custodial” or “skilled.”
Custodial services – like help bathing, dressing, and eating – can be provided by unlicensed and non-skilled care providers. These services may be delivered in a variety of care environments – from your own home, to adult daycares, to nursing homes – but, ultimately, these services are not covered by health insurance or Medicare.
So, you’re stuck paying for these privately (that is, out of your own pocket), through Medicaid (after you’ve exhausted your own assets), or through long-term-care insurance.
Skilled care – that is, the sort of care that is provided by licensed and skilled medical professionals – may be covered by health insurance and Medicare. But this is not always the case because of Medicare’s rules and because it only really covers “curative” interventions – as discussed, above.
Notes:
[1] In terms of whether or not a person would be safe to reside in an assisted living facility, or whether they require a higher level of care, sometimes people talk about various requirements. These are things such as being able to get to an exit by yourself, being able to get around without mobility aids, and so on. I’ll get into greater depth on these questions in subsequent posts or videos.
[2] There are also adult-daycare, hospice, and respite facilities. But I will get into those in another place. See my video presentation, HERE.
[3] Getting into detail about the precise rules, here, is beyond the scope of this article.



















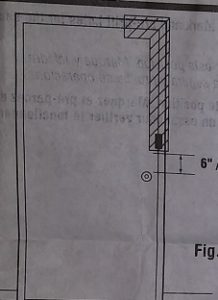


{kind=link}
{kind=link}