The TDP-43 Bridge (Dementia and Cancer)
Historically, medicine has treated neurodegenerative disease and cancer as opposite problems.
In conditions such as Alzheimer’s disease, ALS, and frontotemporal dementia, cells die too soon; in cancer, cells refuse to die — and grow out of control.
These appear to be opposite biological problems. (At first glance, anyway.)
But… researchers are increasingly discovering that diseases we once thought were unrelated may actually have similar explanations — or even the same underlying cellular vulnerabilities.
New research from Houston Methodist suggests that these two “opposites” — dementia and cancer — may share a common root.

The factor being singled out is a protein called “TDP-43.”
For years, researchers have recognized abnormal TDP‑43 accumulation as a major pathological feature in ALS and frontotemporal dementia —
…though its exact role in disease progression has remained unclear.
Suffice it to say that, if doctors find it clumped up in the wrong place in the brain, it’s interpreted as a sign of impending trouble.
But we didn’t have a clear picture of why it was there or what it was actually doing.
As it turns out, this protein appears to play an important supervisory role in how our bodies repair DNA damage.
Today, we’re going to look at how a “glitch” with this one protein “supervisor” can contribute to the breakdown of the brain on one hand, or to the growth of a tumor on the other.
[Video placeholder]
To understand this TDP business, we need to talk about how your body handles its “instruction manual” — your DNA.
Every time your cells divide, they have to copy billions of lines of genetic code. It’s like a clerk typing out a massive book by hand. Inevitably, the clerk is going to make typos. You might get an “A” where there should be a “T.”

Healthy bodies have a “Proofreading System” (scientifically called Mismatch Repair).
Technically, “proofreading” happens during replication in real-time; whereas, mismatch repair is a sort of after-the-fact damage control.
But, in general, this system scans the code, finds the typos, and swaps them out for the right DNA “letters.”
TDP-43 appears to help regulate parts of that proofreading system.
It doesn’t just do the proofreading; it helps coordinate when repair processes activate and how they function. When this system is balanced, your DNA stays more stable.
But the Houston Methodist study found that when TDP-43 becomes dysregulated, the whole system can begin to break down.
Let’s look at this a little more closely.
ALS and FTD
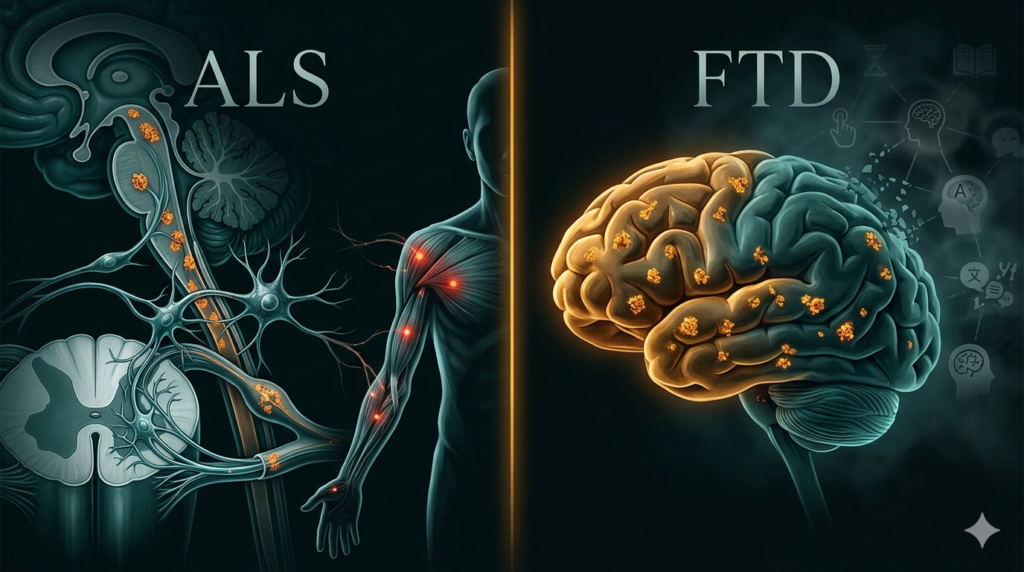
What actually happens in the brain?
Scientists have discussed two cases. The fits concerns the neurodegenerative motor-neuron disease known as amyotrophic lateral sclerosis, “ALS,” or — as I grew up hearing about it — “Lou Gehrig’s disease.” The second case study is frontotemporal dementia, or “FTD” — the latter has been in the news over the last few years due to the tragic diagnosis of famed Hollywood actor Bruce Willis, as we have discussed in other material. [Insert appropriate link(s).]
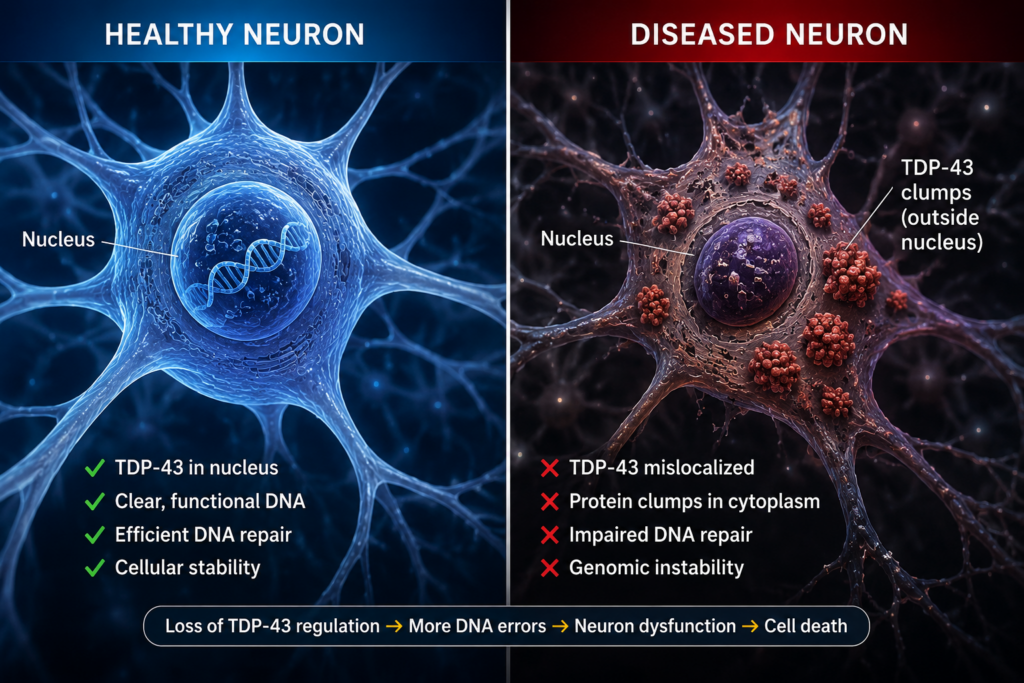
TDP-43 functions as a kind of DNA “Manager.” But, in ALS and FTD this Manager malfunctions.
It stops being where it’s supposed to be (namely, within the nucleus) and it starts clumping together in the “hallways” of the cell. This is the “Missing-Manager” scenario.
When the “manager” is missing or displaced, the repair system can become less coordinated and less reliable. This may allow more errors than usual to creep in, and for instability to build up over time — which, in turn, renders the neuron’s DNA volatile.
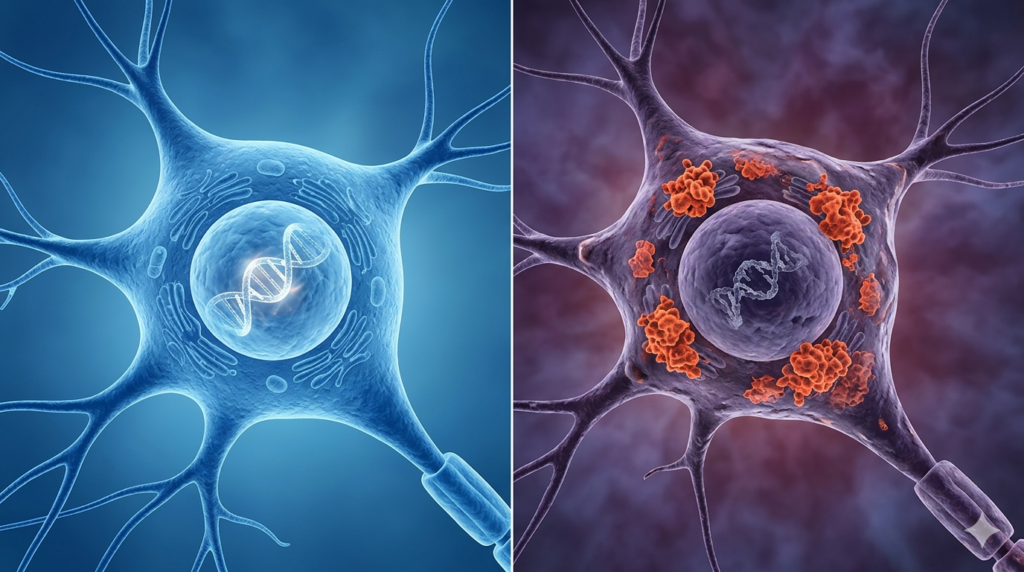
Over time, the cell can’t function because its “instructions” are full of errors.
Eventually, the cell gives up and dies. This mass “cell death” is what causes the symptoms of dementia — memory loss, loss of motor skills, and overall cognitive decline.
Now, let’s look at another side of the TDP-43 problem.
Cancer
Cancer is, at its core, a disease of corrupted instructions. Mutations can push cells to keep dividing, to ignore normal limits, and to survive when they shouldn’t.
The Houston Methodist team looked at large databases of cancer patients and found something striking: in many tumors, there is an over-abundance of TDP-43.
Call this the “Manager-in-Overdrive” scenario.
When there is too much TDP-43, the proofreading department may become imbalanced. This loss of equilibrium can — once again — allow genetic errors to accumulate more rapidly.
By looking at these tumors, researchers found that high levels of TDP-43 were associated with a higher “mutational burden” in multiple cancer types.
This basically means that a particular cancer is changing and evolving quickly.
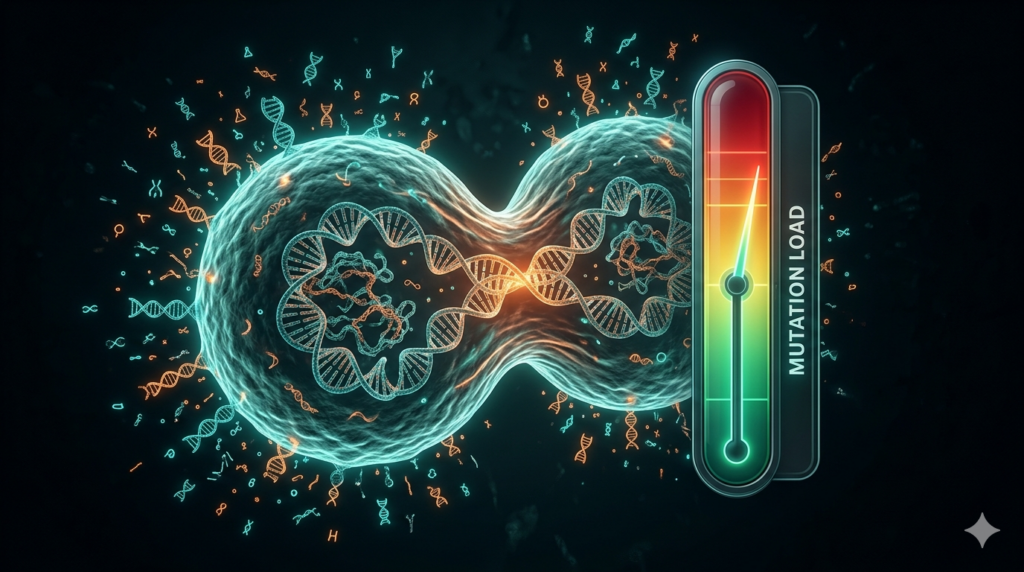
Tumors with high mutation rates can become harder to treat because they may evolve in such a way as to develop resistance to chemotherapy or to evade the body’s immune responses.
So, while too little TDP-43 may contribute to the death of brain cells, abnormally high TDP-43 activity may contribute to tumors growing faster and becoming harder to treat.
This might sound like a “lose-lose” situation, but for scientists, this is actually an incredible opportunity. Before this discovery, we were trying to fix dementia and cancer using completely different tools.
Now that we know (or, at least, highly suspect) that TDP-43 and DNA repair may sit near the center of both processes, we have a potentially unified experimental target.
The findings suggest that restoring balance to these repair pathways could become a future therapeutic strategy. The aim would be to maintain TDP-43 in a sort of “Goldilocks zone”: not too much, not too little.
- In the brain, this could mean protecting neurons by helping keep their DNA stable.
- In cancer, this could mean slowing down the tumor’s ability to mutate, potentially making it easier to treat or more susceptible to a range of traditional therapies.
Caveats and Disclaimers

It’s important to note that this research is still in an early stage, and it’s focused primarily on understanding the underlying biology rather than testing new treatments in patients.
Additionally, both “cancer” and “dementia” are generic terms. This is to say that they range over an assortment of discrete — and, often, highly varied — conditions.
To put it another way, neither “cancer” nor “dementia” is just one, single condition.
Therefore, even if this TDP‑43 mechanism does prove important in — say — ALS and FTD, it does not automatically follow that it explains other dementias, including Alzheimer’s disease.
That said, we are starting to see the beginning of “cross-over” medicine.
Scientists are now looking at whether certain drugs used in cancer research could eventually be modified to help dementia patients — or vice versa.
The big takeaway here is that our bodies are incredibly interconnected.
A protein that we thought only mattered for brain health turns out to be deeply involved in protecting the integrity of our genetic code.
By understanding how TDP‑43 helps regulate DNA repair, researchers may eventually develop treatments that target deeper cellular mechanisms rather than addressing symptoms alone.
Eventually, we may learn how to restore balance to the dysfunctional systems that could be at the center of both cancer and dementia.
The lesson may not be that TDP-43 is “good” or “bad.” Rather, it’s that our biology appears to require a very narrow balance.
Too little may destabilize DNA repair in one direction. Too much may destabilize it in another.
It’s a reminder that in biology — as with a lot of other things in life — balance can be key.

Now, there are plenty of details that I have ignored. And, frankly, many of them may be beyond my ken. But if you want to dive deeper into the technical specifics of the study — I’ve linked the full article from the journal Nucleic Acids Research in the description below.
As a reminder, this channel is mainly focused on the health and science topics relevant for Alzheimer’s Proofing your diet, lifestyle, and — for caregivers — your home environment.
And on that note, I wish you all the best in whatever scenario you find yourself.
Thanks for reading! Don’t forget to check out the YouTube version!
Sources
- Vincent E Provasek, Albino Bacolla, Suganya Rangaswamy, Manohar Kodavati, Joy Mitra, Issa O Yusuf, Vikas H Malojirao, Velmarini Vasquez, Gavin W Britz, Guo-Min Li, Zuoshang Xu, Sankar Mitra, Ralph M Garruto, John A Tainer and Muralidhar L Hegde, “RNA/DNA-Binding Protein TDP-43 Regulates DNA-Mismatch-Repair-Genes With Implications for Genome Stability,” Nucleic Acids Research, vol. 53, no. 18, Sept. 23, 2025 [online], Oct 2025 [print], <https://academic.oup.com/nar/article/53/18/gkaf920/8262242> and <https://pubmed.ncbi.nlm.nih.gov/40985771/>.
- “Scientists Discover Dementia-Linked Protein May Also Fuel Cancer Mutations,” Houston Methodist, via Sci-Tech Daily, Mar. 6, 2026, <https://scitechdaily.com/scientists-discover-dementia-linked-protein-may-also-fuel-cancer-mutations/>.
- For more from the scientists who produced the study, see Houston Methodist, <https://www.houstonmethodist.org/academic-institute/research/>.
- Other writing by Matthew J. Bell, see: Substack, <https://matthewjbell.substack.com/>.