When I was a kid, and I heard “adults” saying: “Oh, they grow up so fast,” I probably rolled my eyes. I mean, how obvious can you get, right?!
Now I have two sons – both in their early 20s. Now I know what “they grow up so fast” means.
Similarly, I didn’t need my dad and grandma to get Alzheimer’s Disease to know that “dementia is bad.”
But it’s a bit like “they grow up so fast.” Sometimes, the things you’ll nod your head (in agreement) to, don’t really sink in until you’ve had a certain amount or type of experience.
So, here’s what I’ll do in this video. I’d like to list five (5) things that probably seem so obvious that I don’t think I ever would have denied them.
At the same time, from where I sit now, I realize that I didn’t actually appreciate the full significance of any of the five until I became the daily caregiver for my dad around 2008.
(The video version of this presentation is available on our YouTube channel.)
My dad died in 2016 from complications related to his Alzheimer’s. I have had several years to decompress and reflect on my family’s experiences with that dreaded disease.
So, I don’t say that just being my dad’s caretaker illuminated my mind. And I won’t pretend that merely listing these things for you will illuminate yours.
At the same time, I feel like encouraging you to slow down and maybe meditate on these things might be worthwhile. So, okay…
Dementia can change your loved one’s entire personality.
If, pre-2008, you’d have asked me: “Can Alzheimer’s alter personality?” I’m sure I’d have said, “You bet.” Nevertheless… Here’s what I thought when I started caretaking.
I thought my dad would continue to be the same extroverted, happy-go-lucky, laid-back person I had always believed him to be. – just with increasing memory problems. It took months – and countless frustrating, tearful, and sometimes (frankly) scary interactions – to learn that Alzheimer’s had flipped his personality. Almost all my dad’s traits that I just listed literally turned into their opposites. He was withdrawn and isolated, combative, agitated, etc.
Now… a case can be made that all these “negatives” had always been there, deep down. Everyone has a “dark side,” kind of thing.
So, maybe, for most of his life he was just really good at hiding or restraining those parts. And, maybe, when he got Alzheimer’s, he just couldn’t or wouldn’t hold back any more. Regardless…
What you “get” – when caring for a dementia-afflicted loved one – is often quite different from what you’re used to, what you expect, and especially what you hope for. So, be prepared for anything! Or, to put it another way, realize that the person you’re dealing with – while they may resemble the one you’ve known and loved your entire life – might act like a complete stranger.
Being a caretaker can make you feel really depressed.
Again, is this a surprise? Even people with no experience with Alzheimer’s probably know that it’s a horrible – and terminal – disease. Watching a loved one deteriorate is depressing.
But I thought that I’d at least feel as if I were doing something worthwhile by helping my dad.
And, don’t get me wrong, it was worthwhile, objectively speaking. In hindsight, I do cherish the fact that I was present for and with my dad.
Subjectively, though, when everything was going on, I felt miserable. Caretaking frequently felt futile and useless. And I felt physically sick much of the time. Maybe it’s just me.
It wasn’t just the understandable fact that my dad didn’t appreciate what I was doing. It was that he resented and actively resisted me. The whole thing was a fight practically from day one.
I locked the doors from the inside. I hid his tools. I disabled the car and – ultimately – pushed his long-time doctor to petition the state to get his driver’s license revoked. I was the enemy.
I knew that the steps I took had to be taken. But it was also painfully obvious my dad was being systematically cut off from all the things that gave him freedom and that he always loved to do.
I tried to remind myself that his disease was really to blame – not me. But that didn’t stop me from being overcome with guilt and regret. I’ve gotten more into all this in a dedicated video.
So: If being a caregiver makes you feel awful, you’re not alone. I felt horrible.
And, on the wavelength of things I didn’t fully know: Know that your life – and the life of your loved one – may be permanently changed. Relatedly…
You will need to take breaks.
Not taking a break can lead to serious consequences – not least is your own emotional or physical breakdown and burnout. Who would deny it?
By the same token, you can’t exactly leave an Alzheimer’s sufferer by themselves for any length of time. It may be difficult for you to prepare and eat meals in peace or to get an uninterrupted night’s sleep, let alone to take a mini-vacation. And this can go on for years.
In our case, my dad would live nearly eight (8) years after his diagnosis. That’s a long time to be someone’s 24/7 caretaker all by yourself.
So… how are you going to take those needed breaks?
As I’ve mentioned in other presentations, if you have no able or willing family members to relieve you from time to time, or in an emergency, then you may have to turn to professionals. Adult daycare, home-care providers, and (what are called) respite-care specialists can all play rôles, here. But, however you get help, you need to make sure that you take care of yourself.
Ultimately, a nursing home or other long-term care facility may be the only game in town. And on that note, try to more fully appreciate that…
Your loved one may end up in a nursing home.
And when I say “end up,” I don’t mean to suggest that it’s inevitable. I don’t believe that.
And, in my case, I don’t mean to refuse responsibility for the decision to get him admitted. It was my choice.
But, honestly, early on, I did a lot of “ostriching.” If I had seriously faced the fact that a nursing home was a possible – or eventual – outcome, I’d like to think that I would’ve planned for it.
I’d say: “I would have planned better.” Except, to be frank, I didn’t do any real planning at all.
No one in my family wanted to think about dad being in a nursing home. – including me.
And I put off any serious thought about that option until I was totally exhausted with caretaking. By that time, our options were severely limited. Even among homes we could “afford” (quote, unquote), our top two (2) choices were unavailable. They both had year-long waiting lists.
And because I was emotionally broken when I started to look into various homes, it’s likely that I didn’t investigate as thoroughly as I might have. – or, quite possibly, as I should have.
Since you can’t reason well when you’re under duress, my evaluation of the options – and my decision – were probably compromised also. It would have been healthier for me to admit, from the get go, that I couldn’t really rule out nursing homes.
If I’d have done only that, our decision-making process would have gone much better – and, possibly, yielded a better outcome. To top it off, I didn’t fully appreciate that…
A nursing home isn’t a perfect solution.
Again, who would say otherwise? For one thing, it’s obvious – at a general level – that when we’re deciding between two or more options, each choice will have positives and negatives.
Duh. Right? In hindsight, it seems pitifully naïve of me to have ever hoped that a nursing home would be “the answer to all my prayers.” Of course, nursing homes have their own drawbacks.
Some of these disadvantages are both major and pretty obvious – like the fact that they have a staggering, current average cost in the vicinity of $8,000 per month.
Another serious downside – one that I intend to make the focus of its own video – is the arguable tendency of nursing homes to over-medicate their patient-residents. I don’t want to go too far down this rabbit trail right now. Let’s just say that – in my opinion – my dad’s nursing home medicated him just to make him docile.
But it was hard for me to understand all this when I was at the end of my rope with homecare. The situation became seriously unmanageable. And I became desperate for an escape route.
So, at the risk of concluding with another one of those aphorisms that’s easy to say, but hard to appreciate or do… Try to stay as clear-headed as possible.
From a practical standpoint, try to have open and honest conversations with every interested person in your circle: from family and friends to doctors, lawyers, and so on.
Solicit advice from as many reputable sources as possible. And run your options past your family “think tank.” Try not to exclude any possibilities.
In two (2), planned, follow-up videos, I’ll expand on some of these ideas and explore related topics like “things I wish I’d known when I started off caretaking.” In the very next installment, already written, I’ll suggest three (3) things that I would do immediately, if I had to be a caregiver all over again.
But if you found something of interest or of use in this video, I invite you to click “Like.” It helps YouTube know that you appreciated the presentation.
If you’d be interested in hearing some of my tips, then please Subscribe to the channel (if you haven’t already) and don’t forget to make sure your notifications are turned on – the “bell” icon.
And if you think someone else might get something out of the video, kindly share the original link on your social media pages.
Either way, though, I thank you for watching.
And I wish you all the best for your caretaking efforts.
Alzheimer’s – and other forms of dementia – are menacing and oppressive diseases.
First and foremost, they take their toll on those who are directly afflicted.
But they can – and do – cause much wider-spread devastation.
Those who have seen it “up close and personal,” know this can include financial, physical, relational, and – for those so-inclined – even spiritual fallout.
I have gotten – and will get further – into those angles in other videos.
But among the myriad negative effects are the various emotional and psychological consequences associated with Alzheimer’s – and with dementia caregiving.
Some of these are widely discussed. At least… they’re addressed in general terms, abstractly.
But there’s an issue that tormented me, personally. Reading comments on some of my videos – especially “When Is It Time For a Nursing Home?” – it seems that I’m far from the only one.
So, in this video, I want to talk about what to do when your caregiving efforts drive you to agonize over the question: Does this make me an awful person?
Caveats
I am not a counselor, psychologist, therapist, or anything close to these. And I am not a healthcare provider or medical practitioner of any kind. Therefore, I cannot diagnose mental- or physical-health conditions, and I am unable to give specific personal advice. If you have depression or thoughts about self-harming or anything in those vicinities, you need to seek professional help. This video is intended for general educational or informational purposes only. I am speaking solely from my own experiences and reflection. And my aim is to raise awareness of these issues as well as foster feelings of solidarity among other caregivers and sufferers. The message is: You’re not alone if you feel this way or have these concerns and doubts.
Ten Reasons Why Being a Caretaker Can Make You Feel Like a Terrible Person
This will be rough-going. I’m going to try (!) not to linger on any point – but just sketch them. As always, your comments are welcomed, especially since it’s a good bet that I missed something.
#1 Missing the Signs of Dementia
If you’re like me, you may have a tendency to punish yourself for not having recognized the evidence of Alzheimer’s, or for misinterpreting the signs that you did see. This may or not be the first thing that prompts you to feel rotten. But, thinking back over my caregiving experience, it was the first thing that I thought of.
As I have explained in several videos, my mom seems not to have recognized my dad’s dementia at all. When I came into the picture, I knew immediately that something was wrong.
But I didn’t understand what I was witnessing. Frankly, I thought my dad had turned into a jerk.
It’s easy to feel bad for thinking ill of him. In retrospect, the temptation is strong to regret not being more intuitive or perceptive or for lack of knowledge.
But REALIZE: Alzheimer’s is a tricky disease. And (as I explained in a past video), even doctors can fail to see the writing on the wall. So don’t beat yourself up! We’re not omniscient, after all.
# 2 Being Unable to Help Them
A major and continual problem is our seeming inability to provide meaningful assistance.
When your loved one is struggling to remember an event or name, you may be unable to convince them of an answer that you know to be correct. And you’ll feel like a failure.
REALIZE: It’s not like helping a non-afflicted person remember something they’ve temporarily forgotten. A normally functioning person can know they’ve forgotten something and, after it’s been brought back to their attention, they can remember what they’re forgotten. Alzheimer’s Disease literally destroys the brain. At some point, a cognitively impaired person may no longer have the forgotten memory or any means to retrieve it.
Even more, we’re powerless to stop the advance of dementia. This is obviously a deeply distressing fact. And even though Alzheimer’s is only one of numerous terminal illnesses, it – and cognitive disorders like it – don’t just kill the body. They kill the mind and the personality.
It’s gut-wrenching when your loved one doesn’t recognize you, or repeats over and over that they wanna go home, when you’ve gone above and beyond to give them a caring environment.
FURTHER REALIZE: That just your calming voice or loving touch is helping them at some level. Yes, you feel terrible when you make a loving home-care environment, but it goes unacknowledged. And, it’s true, once their impairment is far-enough advanced, they probably won’t be able to appreciate your efforts. The most important thing, however, is that you provide an objectively loving, safe, and secured space for them – not that they are aware of your efforts.
#3 Calling in ‘Authorities’
Alzheimer’s sufferers may have outbursts. Some might sob uncontrollably. Others may laugh inappropriately. It’s easy to become distraught when you’re unable to calm or comfort them.
My dad was at the opposite end of the emotional spectrum. He frequently exploded in anger. I had to physically restrain him on one occasion. Just what do you do when things get heated?
I once called a well-known dementia-care support group (that’ll remain nameless). And I asked them this question. Believe it or not, the advice I was given was: Call the police!
…which – after my dad’s next nasty outburst – I actually did.
I’ve no clue whether this suggestion reflected an organizational policy or was just the quirky opinion of the person who happened to answer the phone that day. And I’m not saying the step is never warranted!
But, in my case, the ensuing encounter was thoroughly discouraging – and the intervention was revealed to be obviously unsustainable.
Oh, sure, dad settled down at that moment. But I was made to understand – in no uncertain terms – that the police department had neither the manpower nor the training to be home-care “orderlies.” And it’s not like my dad “learned some lesson” or would even remember the episode.
REALIZE: You do what you can with the data you have. I like to draw an analogy with the daily forecast. If you plan your activities around the expectation of sunny skies – and you did your due diligence: checking the radar and weather report, etc. – and it ends up raining, it’s not your fault. Sometimes the best information available to you is just plain wrong.
Another aspect of this isn’t quite as dramatic. It has to do with your loved-one’s doctor.
As I noted elsewhere, physicians often depend on family members to know that something is wrong with a loved one. In my case, I wrote to my dad’s primary doctor letting him know that my mom, my sister, and I were all extremely worried – especially about the issue of his driving.
Specifically, I had to push the doctor to write a report that resulted in dad’s license being revoked. And that felt really lousy. – like I was going behind my dad’s back and betraying him.
What I had to REALIZE, there, was that other people’s lives and wellbeing were at stake. It wasn’t simply about my dad and his autonomy.
What if he confused the brake and the gas pedal while at our local park? – with families walking everywhere and little kids bike riding, playing, and running all over the place?
No. I felt that – as unfortunate as it was – it had to be done. And, ultimately, it wasn’t me doing anything to my dad; it was the Alzheimer’s Disease that was to blame.
#4 Being Embarrassed by Them
But, of course, when your loved one loses their mobility – or has their autonomy restricted, that doesn’t necessarily mean they simply become homebound shut-ins. – At least, not until the dementia becomes really physically debilitating.
It probably means that you have to pick up the transportational “slack.” And this may not simply range over doctor’s appointments.
If you’re in the position of having to assume caretaking all by yourself – and see my recent video – then you might have to cart them along: As you go shopping and run other household-related or personal errands.
And even if you’ve got help on those fronts, your afflicted loved one will need haircuts. Maybe they gain or lose weight and need to try on new clothes.
You might even want to include them in enrichment or leisure activities. My dad always enjoyed outdoor theater during the summer. My mom and dad had their favorite restaurants. And so on.
But, this can give rise to awkward situations. For instance, I was present at a church service during which my dad caused an obscenity-laced disruption. Several times, he caused a “scene” at local stores. He even picked a fight with a relative during a family reunion over some slight – whether real or imagined – that apparently went back decades.
These sorts of experiences can make you not want to be seen with them in public or take them outside at all.
REALIZE that your loved one may benefit from interpersonal interactions. But, sometimes, events are too busy or loud for a person with dementia. They may easily become overstimulated or overwhelmed. So, if possible, choose events and places that are calm and relaxing.
But what can you do about feeling embarrassed? Firstly, it’s totally understandable. Just ask parents of unruly kids.
Something else that I wish I had done more frequently was to alert people around me about my dad’s cognitive problems. There is one way to do this without making a fuss – and without having to say anything out loud that your loved one might not take well.
Namely, there are little business-card-sized announcements displaying text such as: “The Person I’m With Has Dementia. Please be patient. Apologies for any inconvenience.”
In my experience, most of the time, when bystanders react negatively, it’s because they think that a person who is behaving badly is freely choosing their actions. If you can alert people around that something is wrong, they are often much more forgiving.
#5 Losing Patience With Them
Speaking of this, it’s not always easy for caretakers to remain calm, either. And there’s certainly no shortage of composure-testing situations that can arise in a home-care context.
Providing daily care – including supervision – can become monotonous and tedious. Depending on your demeanor, one of your constant struggles might be losing your temper.
It’s easy to become impatient when you have to say the same things over and over.
Again, child rearing is similar in this regard. But, with kids, at least they’re small and are acquiring the capacities to learn and remember. – Not so with a dementia-afflicted adult.
REALIZE that you might not be able to handle caretaking all by yourself. At some point, you might need to seek assistance. This might mean that you have a heart-to-heart with relatives and ask them to step in – whether temporarily or on an ongoing basis.
But it might also require that you consider professional-care options. As I’ve discussed elsewhere, respite facilities exist to offer family caregivers “breaks” on a short-term basis. And, of course, nursing homes may be the only viable long-term alternatives to home care.
#6 Feeling Your Loved One Is a Burden
Another way to say this might be that you find yourself resenting their decline. I mean…
It’s justifiable, and natural to lament your loved one’s cognitive and physical deterioration.
But what I have in mind is different. It’s that you might find yourself becoming bitter at all the time you have to spend attending to their needs. Or you may develop a “grudge” over the fact that your loved one is unable to appreciate – or understand – your predicament and sacrifices.
Relatedly, you might get depressed – or panicky – at the emotional, financial, or physical strain. This may well include having to take leave from a job and, essentially, to put your life on hold.
REALIZE that you’re only human. Your capabilities and your resources are finite. It’s important – vital even – not to make rash choices. If you find yourself down in the dumps after an especially trying week – or month – then try to give yourself a bit of space.
That’s easier said than done, of course. But, as I have discussed in past videos…
…most recently, the one titled “Is It Possible to Be a Caretaker All By Yourself?” …
…there are a few options available to help you. I’ll defer to some of my other presentations for the details. But you may be able to secure what is called “Respite Care.” This is short-term assistance designed for the sole purpose of giving primary caretakers a much-needed break.
Sidelight: Know (Or Discover) Your Limits
At a certain point in time – it does no good for you to press too far beyond your reasonable limits. I choose my words very carefully. There are three key phrases or terms, there.
“A certain point in time,” “too far beyond,” and “your reasonable limits.”
At the end of the day, only you (and your family) can determine, hopefully in consultation with each other, with friends, and with trusted advisers – like doctors, financial advisers, lawyers, etc. – what these points and limits actually are.
But the flip side of making a hasty decision when you’re temporarily or uncharacteristically emotionally low, is disregarding – or refusing to think about – your limits.
And that can land you in extremely dangerous territory. One sign of this might be, …
#7 Wishing Your Loved One Would Die.
Or wishing that they were already dead. Let’s draw a few distinctions.
Number one, there’s a difference between (on the one hand) lamenting that your loved one is suffering – focusing on their pain for their sake – …
…and (on the other hand) worrying about their pain because of how upsetting it is for you. – whether for you to deal with, or for you to witness at all, or… whatever.
My dad wasn’t diagnosed with Alzheimer’s Disease until the summer of 2009. Immediately preceding that diagnosis, my dad had had two major surgeries just a couple months apart.
On the eve of the first – a triple bypass – my dad was literally on death’s door. Those surgeries prolonged his life for seven years, as it turned out.
But, it’s easy to ask: For what?! Those years were dominated by cognitive decline. I spent four of them caring for him at home, and he spent his last three in a nursing home.
I regularly found myself wishing, or at least, wondering: If only he had died in 2009!
Don’t get me wrong: On my better days, what I was mainly thinking was: If only he had died of a heart attack, his death would have been relatively quick (in theory)… and he would have been spared a near-decade of slowly wasting away – both mentally and physically.
There is space, here, for a discussion of various spiritual perspectives. I’ll leave that complicated topic for a possible, future video. But REALIZE: You can’t control what life gives you; you can only control how you react or respond to it.
Granted, it’s easy to say and hard to do. And I confess: not every thought I had was “altruistic.”
So, number two, we also want to distinguish between a fleeting “bad” thought and an all-consuming idea. Admittedly, there’s a vast middle ground between the two extremes.
Anyone might be susceptible to having the occasional selfish desire. You want to guard against obsessing over such thoughts. For me, this came when my dad was in the nursing home.
Towards the midpoint of dad’s nursing-home stay, we had our first dealings with hospice.
“Hospice” is end-of-life, palliative care for terminally-ill patients. Every time we’d get a call that dad was being “put on hospice,” the news hit us as if he’d just been handed a death sentence. Obviously, I’m speaking loosely. The late-stage Alzheimer’s itself was the real death sentence.
We just didn’t realize that a person can see-saw on and off hospice. Roughly half the time dad was in a nursing home, my family was on edge, expecting that his death might come any day.
That is exhausting, to say the least. Your emotions are like a yo-yo. And it can be both financially and physically demanding.
For example, the first time you think your loved one is at the point of death, you cancel appointments, you take off work, and you otherwise bend over backward to be present as much as possible. If and when they recover, you’re relieved – and not a little surprised, frankly.
But then it happens again. And again. And again. Finally, you worry how you can keep doing this. And you’re basically stuck. If you do react to every wave of hospice as if it were going to be your loved one’s last minutes on earth, then you can place an ever-increasing burden on your family – depending on how many cycles they go through.
After all, it’s not easy to set aside a year, two years, or whatever to be a part of some protracted, open-ended hospice scenario. Sad, but true.
But if you don’t respond, then you risk not being there when your loved one actually passes. You don’t want them to die alone. So, more than once, I wished he would just die. Because I’m here this time. Or my mom is with him right now. Or my sister is visiting from out of town. If he pulls through again, I don’t know which of us will be present next time.
The thing to REALIZE, here, is that we’re only human. The best you can do sometimes, is to take things one day at a time. Have an honest and open dialogue with the hospice and medical staff about your loved one’s situation. And try to plan (as best you can) for rainy-day scenarios.
Regardless of what stage of care you’re in, and where that care is being delivered, try to nip any selfish thoughts in the bud as soon as they pop into your head. Again… easier said than done.
It may help to focus on why you’re doing this. Think about positives – like happy memories. Try to “reframe” the situation, or look at the end-of-life process as a series of opportunities to spend a few more precious moments with your loved one than you thought you’d get.
If you’re in a home-care situation, then consider whether these thoughts – especially if they’re preoccupying you – might be signs of an impending breakdown. Be honest with yourself.
That includes reaching out for help if and when it’s necessary. It might mean that you seek counseling or arrange for respite or hospice care for your loved one.
It doesn’t do any good to simply bury or deny your feelings. The overall caregiving may suffer – which would be bad for your loved one and for you. And that leads to the next consideration.
#8 Regretting Your Caretaking Decisions
It’s an understatement to say it, but …the caretaking road is tiring.
It may also be long and winding. You may feel like you’re wandering lost with no clue how long it will take you to arrive anywhere – or to get back.
You may have mounting debt or expenses. You yourself may be developing age-related physical problems at the same time your loved one is declining. These – and other – factors can lead you to wonder: Can I do this at all? Or …Can I keep doing it?
You can get the distinct impression you’ve bitten off more than you can chew.
And that can lead you to think you made the wrong choice – or a bunch of wrong choices – somewhere along the way. I want to tackle that worry head-on in another video.
But if you start thinking that it was a mistake to take your loved one in, or to assume caregiving responsibilities in the first place, then it can throw you into a spiral of self-doubt.
REALIZE: You’re not alone. Probably every caretaker will harbor similar concerns if they are at it long enough. While this won’t necessarily allay fears that you took a wrong turn, I say it because it’s arguably never clear to anyone what the “correct” path is. You consider your loved one’s well-being of paramount importance, you gather information, you talk your options over with trusted friends and advisers, and you try to do the best you can with the hand you’re dealt.
If, ultimately, things become unmanageable, that may lead to you having to course-correct.
#9 Having to Institutionalize Your Loved One.
And that leads me to this next item. Let me come at this by way of a recent comment. Let’s just say that the opinion was acerbic.
The commenter wrote, in part: “ …I cared for my wife on my own… It did not occur to me to farm her out to await death to make my life more comfortable. …”
Honestly, I doubt that the commenter watched my video. Instead, it seems that he was merely reacting to the title. It’s possible that he misconstrued “When Is It Time for a Nursing Home?” as me saying that – eventually – every caretaking scenario will end with institutionalization. – Which, of course, I don’t believe is true and never said.
Either that, or else he objected that anyone would ever admit their loved one into a nursing home. It’s a view that treats the nursing-home option as tantamount to throwing in the towel (at best) or seeking the easy way out (at worst).
For our purposes, I’m highlighting this because it might easily be taken to heart as an indictment of a caretaker’s commitment to his or her loved one. – As if the only way to show love is to assume full caregiving duties – and stick to them – come hell or high water. Since I turned to professional care, that makes me a bad son.
REALIZE that no one has walked in your shoes. No one should impugn someone’s else’s familial love on the sole basis of their having to utilize a nursing home.
If we didn’t care, we wouldn’t be anguishing over the decision.
But not only is a comment like this uncharitable, it’s really incomprehensible. It half-implies that nursing homes should never be an option.
As many of you know all too well, it’s not always possible – emotionally, financially, physically, or whatever – for family members to be at-home caretakers. In fact, if a better, more complete, kind of care can be delivered in a skilled-nursing facility than in a home, then you could turn the poster’s allegation around and say it would be unloving not to use the nursing home.
Personally, I believe that things are often much more complex and nuanced than either of these dismissive reactions would suggest. For one thing, nursing homes may (or may not) offer quality care. This is just to say that the way forward is not always obvious. In fact, I’d be hard pressed to find a case where the “right decision” is obvious!
No …If there’scertainty in any of this at all, it’s that there is no one-size-fits-all approach.
Thankfully, though, you and I have nothing to prove to anyone else. At the end of the day, it’s for you – in consultation with your support network – to make the best decision you can for your loved one and for your entire family.
#10 Finding That You Don’t Feel Anything at All
Up to now, we’ve been trying to come to terms with various experiences that can make you feel miserable. And that unhappiness can make you wonder if you’re an awful person.
But what happens if you don’t think you’re feeling anything at all?
Someone might hear me explaining how I was tortured over things like the decision to admit my dad into a nursing home or how I was periodically embarrassed by him in public, and so on.
And it’s perfectly imaginable that somebody might think: I’ve never felt anything like that. Does that mean I’m a horrible person?
REALIZE that people deal with adversity differently. I tend to be a reactive, volatile person. I can get worked-up easily.
So, don’t compare – and certainly don’t judge – your emotional reactions to mine or anyone else’s.
But also REALIZE that not feeling anything can mean a lot of different things. For example, it might mean that you’ve become emotionally numb. Caretaker burnout is a real danger.
Remember, also, emotional flatness can be bound up with the so-called “denial stage” of grief processing. So, as I stated earlier, just be willing to be honest with yourself. You might need to take a break. Or you may need professional help – whether for your own mental or physical well-being or for assistance with the day-to-day business of caretaking.
Concluding Remarks
Being a caregiver for someone with dementia can make you feel a lot like Sisyphus. You’ll recall that in the Greek myth, Sisyphus is fated to push a rock uphill for all eternity. Every time he manages to reach the summit, the rock rolls back down the mountain and he has to do it again.
It’s frustrating. It can feel altogether absurd and futile. Additionally, some of the caretaking measures you may need to implement can feel like betrayals. That can be depressing. And it may lead you to feel inadequate, unworthy, and even wretched.
Recently, I realized how many times in past videos I say something like “it sounds bad, but…”.
Why install double-keyed deadbolts on the entry doors? It sounds bad, but… it’s so your loved one can’t easily get out of the house.
How hard is it to care for someone with middle-stage dementia? It sounds bad, but… caretaking can be more manageable if they’re also physically disabled.
I was racked with guilt after having my dad admitted into a care facility. I had nightmares for years afterwards. And it sounds bad, but… the worst were bad dreams in which my dad came back to the house and I was once again thrown into a stomach-churning hopelessness.
You love your afflicted dad, mom, grandparent, spouse, …or child! They’re not actively doing anything to you. They’re not intentionally making you miserable or “oppressing” you.
And you know they’re suffering, too. As my sister said to me during one heart-wrenching exchange in which we discussed institutionalization: Dad is himself in a really bad place.
That’s an understatement, of course.
Trying to imagine what it was like for him is, frankly, sickening. You’re “stuck” inside a body and with a brain that can’t or doesn’t or won’t cooperate with you?! I picture being locked in a windowless room – cut off from others and, eventually, from myself. It’s horrible, hellish, in fact.
Deep down, we know all this “full well,” as the saying goes. That’s the point. The enormity of the pain – on all sides – can be terrifying. Even so, you want so badly to continue to believe that – in their “heart of hearts” – your loved one cares about you, still remembers you, still loves you.
In a sense, it’s precisely that belief – and that hope – that adds insult to injury.
Because… You desperately want to help them. But when they’re cursing you out and throwing things around the house; or when they don’t recognize you and they react to your caretaking as if you were an intruder; or when they refuse to bathe or toilet and you’re routinely cleaning feces off the carpet; you are thoroughly demoralized.
The situation creates an almost impossible tension. You’re sick over the prospect of nursing-home confinement. At the same time, you can feel like you can’t go on and on like this – or you will literally go insane or totally break down physically yourself.
This psychic pressure can build to the point where your mind goes in really dark places.
I’ve been there.
I don’t want to leave this on a negative note.
Please know that I truly, truly, truly empathize.
If you’re presently going through a hard time, then I invite you to share your experiences and thoughts in the comments.
And if you went through a similarly harrowing journey in the past, then I’d ask that you share as well. I have seen really beautiful exchanges in the comments. And I sincerely believe that people who are experiencing self-doubt – or loathing – can benefit from reading about what other people have undergone – and survived.
I hope that – if nothing else – this video encourages you that you’re not alone. And, sometimes, knowing that is about all that keeps you going. I wish you all the best. Thank you for watching.
People can end up in nursing-home and other long-term-care environments for any of several reasons. And residents may run the gamut in terms of their levels of awareness and disability.
When a resident retains his or her reason, then – in principle – he or she can “advocate” for themselves in the sense of communicating their desires and needs to facility administrators and staff. But what about cognitively impaired residents, such as those with Alzheimer’s Disease or some other form of dementia?
Such persons may require additional assistance. And this is where a Family Council can come in.
Long-Term-Care Resident Groups
Residents in long-term-care facilities, and families of people residing in such facilities, have the ability to form groups. These groups are often organized to facilitate discussions focused on resident needs and facility changes that may have to do with quality-of-care and quality-of-life issues.
As it happens, these groups, when formed, have tended to be referred to as “councils.” There are two main types of these councils that may be created: family councils and resident councils.
Resident Councils
The most basic variety of long-term-care group is going to be the resident council.
In general terms, a “resident council” is an association of individuals who live in a particular care facility and who wish to work together for the enhancement of their shared living experience.
When they exist, resident councils are independent of the care facility. To put it another way, the resident councils are not controlled or run by the facility administrators or staff.
I say that this sort of group is the “most basic” because it is natural for facility residents to provide feedback and input that pertains to their living conditions. They are interested in the facility, not simply in a psychological sense, but in an economic sense – that is, they have an interest in the policies and procedures of the relevant facility.
Family Councils
A related type of long-term-care group is the family council. As the name implies, “family councils” are groups organized and run by families (or close friends or representatives) of nursing home residents instead of the residents themselves. These family members then join with other families and speak for residents in advocating for policy and procedure changes that improve daily care and quality of life.
It should be said that nothing prevents residents from joining or participating in family councils.
Relatedly, I note that the point of the family council is not to compete with, replace, or supplant the resident council.
Rather, the point is to offer assistance to residents. And, the focus of this website being what it is – namely, Alzheimer’s Disease – it is important to observe that this assistance is especially necessary and valuable in cases where residents lack the ability to speak for themselves because of cognitive impairment, dementia, or similar conditions. (More on this, below.)
Brief Council-Related Questions and Answers (Q&A)
What Do Councils Do?
Both family and resident councils may bring to light issues surrounding care and living conditions. These may include, without limitation: the availability of food, medical equipment, silverware; the cleanliness of the facility; the functionality of things such as elevators; the reliability of internet access; and so on.
Essentially, any topic that impacts the quality of life of residents is fair game.
Once topics have been discussed, it is up to the individuals in the council as to how to proceed. Many facilities (see further on) are required to provide the council with a go-between or contact so that concerns can be delivered to the administration or staff without delay.
Councils may decide to bring their concerns to the facility orally or in writing – in a small group or via a designated council representative.
The first and preferable route would be to communicate with the facility.
However, if the facility is unreceptive for whatever reason, or if it somehow fails to satisfactorily address the expressed concerns, then councils may contemplate or undertake other actions.
Are Family Councils Only Allowed When Residents Have Dementia?
No. Family councils can be formed in order to support any person residing in a particular long-term-care facility, whether the resident is impaired or not.
However, it’s arguably even more important for a family council to be formed when resident loved ones do have cognitive impairments, since dementia sufferers may be unable to speak for themselves.
What Are Examples of Conditions That May Result in Cognitive Impairments?
What If a Resident Has No Living (Or Interested) Family Members?
Residents may give permission to non-family members to participate in family councils on their behalf.[1] If a resident has a cognitive impairment, then things can get a little dicey. If you would like a non-family member to represent your interests in a family council, you may wish to record your wishes in writings prior to the manifestation of any condition that might call in question your mental fitness.
Are Long-Term-Care Facilities (Such as Nursing Homes) Required to Recognize Family Councils?
I will address this question at greater length in a forthcoming post.
But, for now, suffice it to say that Federal regulation (in Title 42 CFR 483.10) states that Medicare/Medicaid-participating nursing homes must recognize family and resident groups when they form.
Further, these facilities have to provide resident and family groups with private meeting spaces, and they need to take reasonable steps (with the approval of the groups) to make residents and family members aware of upcoming meetings in a timely manner.
Additionally, the facility must provide a designated staff person to act as a liaison to the group. This person will be responsible for providing assistance to the group and with delivering (though not necessarily writing) responses to formal requests that result from the group meetings.
Does the Long-Term-Care Facility Have to Respond to Council Requests?
The facility cannot ignore the group or suppress its ability to form. So, in this sense, yes, the facility must provide some sort of reply to a group when it is asked to do so.
This does not mean, however, that the facility is compelled to do precisely what the council requests.
Things are tricky. I will try to explore some of these issues at greater length in a future installment.
Six Characteristics of a Family Council
It may be helpful if I briefly sketch some of the qualities that a family council will have.
Autonomy
Autonomy refers to the fact that the group is self-led. Neither a family council nor a resident council is created or led by facility administrators or staff members. If the facility has started and controls a group, then it is not a family or resident council in the relevant sense – regardless of what the facility calls it.
Facilities are of course free to form their own groups; and residents or families are free to join these facility-created groups if they choose to do so. But the formation of a facility-led group is not a replacement for an autonomous family council, and joining a facility group does not bar a person from joining an autonomous group.
Facility Specificity
There may be groups that support anyone living at any nursing home. However, a family council is relative to a specific facility. The ties that bind the members of a family council have to do with the fact that members all have relatives who live in the same long-term-care facility.
Independence
Independence is an extension of autonomy. The administration does not have claims over the family council. The councils are not dependent upon the facility. Moreover, the council is not considered to be a government program. It is an independent association of families of people living at a particular facility.
Interest
A family council must be made up of a group of people who have an interest in the facility. In this context, “interest” does not simply mean a curiosity. It means there has to be an interest in more of an economic sense. Member families have to have some “stake” in the facility and, going further, in the standards according to which the facility operates.
Openness/Inclusivity
There must be no barrier to entry into the family council other than having a close friend or relative involved in the facility. The council be must inclusive or open in terms of its membership.
Privacy
The group is owed a private space that should be provided by the administration of the facility on the facility grounds. The facility cannot appoint a staff member to “sit in” on the meetings.
Administrators or staff may be invited by the group to attend meetings. But, apart from such an invitation, presumably furnished by a council officer or spokesperson, the group should be allowed to meet privately.
Once again, the facility may endorse or sponsor other, staff-led groups. And these groups may also listen to complaints or solicit feedback from families and residents. But, the existence of such facility-controlled groups does not undermine the ability of residents and families to form their own councils to advance their own interests.
Notes:
[1] Presumably, if there is a conflict, a resident could also revoke a family member’s permissions or otherwise “block” one of his or her family members from participating in a council.
Within the United States and Canada there are laws that require a physician to report a patients with neurological or cognitive disorders to a licensing agency, as those patients may be a danger behind the wheel of a vehicle.
This type of reporting is not mandatory across the entire United States. Currently, there are only six (6) states that mandate a physician to report on a patient’s ability to operate a motor vehicle. These six states include:
California
Delaware
Nevada
New Jersey
Oregon
Pennsylvania
Not all mandatory states direct their reporting law toward those who are afflicted with Alzheimer’s Disease or, indeed, any sort of dementia whatsoever. Below are some specifics around each mandatory state and what is defined in their law.
If you want to see and hear me present the material, feel free to watch the YouTube video that I prepared, here:
California
The state of California is the first that I will discuss. It’s a prime example of a state in which (a.) there is mandatory reporting, and (b.) that reporting is at least partially concerned with Alzheimer’s Disease expressly.
The California Legislative Information website (leginfo.legislatures.ca.gov) references chapter 3 – Disorders Characterized by Lapses of Consciousness [103900-103990].
103900 states: “Every physician and surgeon shall report immediately to the local health officer in writing, the name, date of birth, and address of every patient at least 14 years of age or older whom the physician and surgeon has diagnosed as having a case of a disorder characterized by lapses of consciousness.”
This law specifically includes Alzheimer’s Disease as a disorder that involves the requisite “lapses of consciousness.”
In Delaware, the focus is on conditions that are characterized by “losses of consciousness.” In this respect, Delaware’s statutory language is similar to the “lapses of consciousness” verbiage present under California law.
Title 24 of the Delaware Code Online – Professions and Occupations Chapter 17, Medical Practice Act states: “Every physician attending or treating persons who are subject to losses of consciousness due to disease of the central nervous system shall report within 1 week to the Division of Motor Vehicles the names, ages and addresses of all such persons unless such person’s infirmity is under sufficient control to permit the person to operate a motor vehicle with safety to person and property.”
Again, for further reading, scroll down to “Delaware’s entry, HERE.
Nevada
Nevada is a good example of a state in which, while there is mandatory-physician reporting, it is not directed towards cognitive impairments such as dementia (of which, as we know, Alzheimer’s Disease is the most common variety). (On two ways of understanding the difference between Alzheimer’s Disease and dementia, see my YouTube video, HERE.)
According to the Bradley, Drendel & Jeanney law firm: “…Nevada laws can regulate the driving rights of individuals with epilepsy. In fact, doctors in our state are required to report epileptic seizures to the state’s Department of Motor Vehicles…”
You might be picking up on a recurring theme, here, but… for additional information, click down to “What does Nevada State Law say about Driving with Alzheimer’s?” in my 50-State Guide, HERE.
New Jersey
The New Jersey Academy of Ophthalmology, states, “NJ Law (N.J.S.A. 39:3-10.4) requires all physicians to report patients to the Motor Vehicle Commission within 24 hours after determining that a patient experiences any of the following: Recurrent convulsive seizures, recurrent period of unconsciousness or impairment, or loss of motor coordination due to conditions such as, but not limited to epilepsy in any of its forms which persist or recur despite medical treatment.”
Even so, New Jersey appears to be one of those states in which physicians could potentially be held liable, legally, if they don’t report potentially dangerous drivers.
While New Jersey law has established an elective reporting system for drivers with vision deficiencies and mandatory process for reporting specific neurological dysfunctions, there is no statute that protects a physician from liability if they have failed to report a patient that may cause injuries to a third party due to a condition known by the physician.
Given this, you might think that a New Jersey doctor will err on the side of reporting. And, I may be inclined to agree.
For more info, where do you think I’ll send you? My state guide, of course! Find it, HERE.
Oregon
The Oregon Driver & Motor Vehicle Services states: “Most medical professionals are required to report drivers who can no longer drive due to impairment.”
It is required of medical professionals to report on a patient’s impairment, even if that patient has agreed to give up driving.
The Oregon Secretary of State website similarly states: “…mandatory reporting by physicians and health care providers of those persons with severe and uncontrollable cognitive or functional impairments affecting a person’s ability to safely operate a motor vehicle.”
Cognitive impairments as specified in Oregon include: attention, judgement and problem solving, reaction time, planning and sequencing, impulsivity, visuospatial, memory and/or loss of consciousness or control.
Intuitively, this list is expansive enough to range over various cognitive impairments like dementia and Alzheimer’s Disease, even if they are not singled out for special or explicit attention.
See: “What does Oregon State Law say about Driving with Alzheimer’s?” which is a subsection of my longer, and more comprehensive (but certainly not exhaustive) reference, elsewhere on this website.
Pennsylvania
According to Schemery Zicolello Law Firm, the Pennsylvania Medical-Reporting Law requires health care personnel to report to the Pennsylvania Department of Transportation the full name, date of birth and address of every person over 15 years of age that is diagnosed as having a disorder or disability that could impair his/her ability to drive. In the list of reportable medical conditions, the attorneys specifically call out dementia.
That’s good enough for me.
If you want a bit more detail, scroll down to “Pennsylvania,” on my article, HERE.
Utah
Utah was mentioned in an article by National Center for Biotechnology Information (NCBI) as a reporting state. However, in the Fact Sheet for Patients and Families provided for Utah drivers, the indication for mandatory reporting by physicians is not present.
The document does state that the patient is expected to report and disclose their impairments to the department of motor vehicles.
So… I don’t find that Utah is actually a mandatory-reporting state.
Bear in mind that just because a state does not have mandatory-reporting laws, it should not be assumed that physicians won’t report anyway.
In the first place, a doctor might believe that it is his or her ethical duty to report a potentially dangerous driver – regardless of whether state law strictly requires that he or she do so.
Additionally, the physician’s other professional entanglements – for instance, his or her affiliation with a medical group or his or her professional-liability insurance – might have stricter requirements governing action steps in relevant cases.
Mandatory Medical Reporting Law States: In some states, physicians are required to report patients who have specific medical conditions (e.g., epilepsy, dementia) to their state Department of Motor Vehicles (DMV). These states generally provide specific guidelines and forms that can be obtained through the DMV.
Physician Reporting Law States: Other states require physicians to report ‘unsafe’ drivers to their state DMV, with varying guidelines for defining ‘unsafe.’ The physician may need to provide (a) the patient’s diagnosis and (b) any evidence of a functional impairment that can affect driving (e.g. Results of neurological testing) to prove that the patient is an unsafe driver.
Physician Liability States: Case law illustrates situations in which the physician was held liable for civil damages caused by his/her patient’s car crash when there was a clear failure to report an at-risk driver to the DMV prior to the incident.
On the NHTSA’s website, a survey of medical review practices can be found that indicate while all 51 jurisdictions accept reports of potentially unsafe drivers from physicians, only 6 jurisdictions require physicians to report drivers to the motor vehicle agency.
Another helpful article on NHTSA’s website is ‘Current Screening and Assessment Practices’. This article summarizes the legal requirements in each of the six mandatory reporting states.
Another helpful resource is the National Center for Biotechnology Information, the website for which can be found, here: https://www.ncbi.nlm.nih.gov.
National Library of Medicine, National Institutes of Health contains an article within the Journal of General Internal Medicine (abbreviated “J Gen Intern Med”). Of interest is an article titled “Reporting by Physicians of Impaired Drivers and Potentially Impaired Drivers,” which mentions that virtually all states have established policies for the identification of drivers with physical or mental impairments, however, the reporting is voluntary with the exception of specific states.[1]
Additional references on AlzheimersProof.com include:
This is a resource regarding the legalities of driving with Alzheimer’s or another cognitive disorder. This is not legal advice, simply research and research leads presented in a comprehensive article to assist in locating additional sources for further information. You can find additional information and important aspects specific to your state within my 50-State legal guide, HERE.
The above article, also on my website, goes into a discussion about a number of factors that may impact a person’s ability to drive, given their cognitive or mental state. This not only addresses that Alzheimer’s Disease occurs in stages (for more on which, see HERE), but also addresses some concerns around other cognitive impairments.
I also have an article – and a companion video (see my YouTube channel, HERE) – talking specifically about considerations of driving safety, apart from an explicit discussion on any legal requirements.
Now, if it gets to the point where you have to actually restrict your loved one’s access to the vehicle (and I sympathize with you if this happens), then you might find something of use in the above resource.
The final piece that I’ll note, here, is a general article that I did on the question of how to “Alzheimer’s Proof” a car. Recall that Alzheimer’s Proofing is akin, in this context, to baby proofing or childproofing. For more on this, see HERE.
Disclaimer
Please note – this article should not be treated as providing legal or medical advice, but purely as a reference that provides general information in regards to the laws that require a physician contact a licensing bureau in regards to a patient’s ability to operate a vehicle. This post is given as-is; I do not warrant that the information is accurate or complete. But I provide the information in good faith and I believe, to the best of my knowledge, that it is reliable.
Notes:
[1] As noted in the main text, the article’s list of states includes Utah, while in other references, Utah is not mentioned as a mandatory state.
Alzheimer’s Disease is a progressive, neuro-degenerative illness that presents itself in stages. While there is some debate over the precise number of stages (for more on which, see my ARTICLE or companion VIDEO), for present purposes, we can say that there are three: early, middle and late. Because cognitive degradation is just what it is to have some form of dementia, the fact is, at some point, an Alzheimer’s sufferer will become unsafe behind the wheel of a car.
In the early stage of Alzheimer’s, memory impairments may be mild affording a person the ability to safely drive. A larger concern occurs during the transition from the early to middle stage of the illness.
During the middle stage of Alzheimer’s, memory impairments may become more severe. You or your loved one may be doing fine one day, but have a lapse in memory or judgement, causing challenges the next day. These lapses, or deterioration in memory, can make a person with Alzheimer’s more of a danger to themselves or others, especially when driving.
By the time a person reaches the late stage of Alzheimer’s, he or she will have lost so many abilities (including language, mobility, responsiveness, etc.) that driving will be virtually inconceivable. Generally, by that time, the level of physical disability alone makes operating a motor vehicle practically impossible.
But before that threshold is reached, it may be somewhat difficult to identify the precise time at which a person becomes an unsafe (or at least unreliable) driver. Here is a breakdown of some early signs or symptoms that may indicate it is no longer safe for a person with this illness to operate a vehicle.
(These signs may be noticed by the person themselves, a loved one, vehicle caretaker or an outside party such as a neighbor, physician, police officer, etc. Additionally, it is important to assess behaviors and signs relative to a person’s “baseline.” In this context, a baseline is the starting point for comparison. It’s basically the way a person acted or the degree of functionality they possessed for most of their adult life – at a point when they were obviously not impaired in the relevant sense.[1])
Emotional Changes
A person with a mild demeanor may become more aggressive, hostile, or otherwise difficult. These changes in behavior could potentially be due to a mood disorder or other neurological problem. However, these behavioral changes can also occur in a person with Alzheimer’s Disease or some other form of dementia.
If you notice that you or a loved one becomes unable to control anger or depression, becoming so overcome with emotional fits or episodes, it may be an indicator of Alzheimer’s or some other serious condition. Whatever the cause, these emotional changes will increase the dangers and risks of being behind the wheel of a car.
Anger – Your loved one may become agitated or irate with little or no apparent provocation, or beyond what a normally functioning person would think of as justified or reasonable.
Anticipation – In this case, the pathological component may be another outgrowth of memory loss. If you loved one seems or professes to expect or hope for an imagined or past event, it may be a sign of worsening dementia.
Disgust – An Alzheimer’s patient may have difficulty masking emotions and might display naked aversion, distaste, loathing, revulsion, etc. even in inappropriate contexts or directed toward things that they previously felt fondly toward.
Fear – On a low level, this might result in an increasing level of anxiety. It could be apparent through spoken language, but it may only become apparent to people who notice subtler signs or body language (e.g., in facial expression or posture) or habit (such as hand wringing or nail biting). Alternatively, fear may manifest in more extreme ways, for instance, through indications of a pathologically paranoid or suspicious turn of mind.
Joy – We all like to see our loved ones content and happy. But, in some cases, the level of jubilation or excitement may exceed what is appropriate to or warranted for the occasion. For instance, your loved one may not exercise due restraint. Alternatively, it may appear strike you as inappropriate in the sense that he or she seems to be taking pleasure in something that ought to elicit a different emotional reaction.
Sadness – A dementia-afflicted people might suffer from apathy or depression, or from some other related sort of unrelenting melancholy. They may tend to brood or become removed or withdrawn from family or other social circles.
Surprise – Look for evidence or amazement or bewilderment that seem out of place. Astonishment or shock could be a result of affected judgment or reasoning. But it also could be a function of increasing forgetfulness and impaired memory.
Trust – This may be related to fear and paranoia in the sense that your loved one may begin to suspect family members of plotting against them. Contrariwise, it might be expressed in an inappropriate or unwise willingness to follow or receive instructions from strangers.
Memory Changes
Some Alzheimer’s-afflicted individuals may have issues with short-term memory loss but are able to remember things that occurred further back in time. Vehicle operations can be broken up into “before,” “during” and “after” categories to determine if memory changes impact or undercut safe driving. Here’s what I mean.
Before Getting Into the Vehicle, Ask…
Do you or your loved one have an issue finding the keys?
Is it consistently a challenge to remember where the vehicle is parked? Or…
Is it hard to recall which vehicle belongs to you?
Everyone misplaces things from time to time. Obviously, when it is sporadic, this is not necessarily an indicator of Alzheimer’s Disease or some other form of cognitive impairment or dementia. However, the issue occurs when this becomes more of a pathological condition where memory loss is more frequent than normal, or when its occurrence undermines safety.
While Inside of the Vehicle, Ask…
Do you or your loved one have trouble remembering which pedal is the accelerator and which is the brake?
Is there confusion on what traffic signs or signals are indicating?
Do you or your loved one regularly forget where you are going, or how to get there?
Beyond the perceptual diminishment that often accompanies normal aging, cognitive impairments may erode sensory faculties. Does the driver have reduced sensory-processing capabilities? (See further below.)
Do the A/C or radio controls confuse you or distract you from the road?
A person with this illness may not understand signs to where they inadvertently drive through a construction zone. They may also forget where they are going or how to get where they are going, even if the route is familiar.
After Exiting the Vehicle, Ask…
Are there dents or scratches that cannot be accounted for?
Is parking haphazard or erratic?
Are items forgotten inside the car inadvertently?
Are keys routinely left in the vehicle?
Is the car left running unintentionally?
Have you or your loved one begun to receive mailed traffic citations? Or…
Is the driver being pulled over more frequently than before?
A person afflicted with this some form of dementia or other cognitive difficulty may not remember how a particular dent or scrape appeared on the vehicle.
All these items are warning signs or indicators that something else may be going on beyond normal forgetfulness.
Motor-Skill Changes
Cognitive disabilities are only half of the picture, though. Driving also places physical demands on a person. Therefore, various physical impairments can also undermine safe-driving abilities.
Similarly to the previous category, these changes can also be evaluated by looking at requirements that impose themselves before, during, and after using a vehicle.
Before Getting Into the Vehicle, for Example…
Changes in motor skills or reductions in physical strength may hinder a person from doing something as simple as opening or closing a vehicle door.
You or your love done may struggle with opening or closing the hatch or trunk.
It may become difficult or practically impossible properly open or close the hood of a vehicle.
It is true that memory may come into play here as well. And there’s little question but that forgetting how to do these minor tasks may be an indicator of Alzheimer’s.
But diminished motor skills can be serious problems on their own. And, when determining a person’s driving fitness, physical abilities need to be assessed alongside cognitive ones.
While Inside of the Vehicle, for Example…
A person with diminished motor abilities may have difficulty turning the wheel.
He or she may have trouble physically depressing the pedals or shifting gears.
Someone might find it physically taxing to keep the car in the correct lane.
Parking the vehicle may begin challenging, especially if the individual has limited abilities to turn their body or head.
Sensory impairments such as hearing or vision loss can also undercut the ability to safely operate a car or truck.
After Exiting the Vehicle, for Example…
Do you or your loved one have difficulties just physically getting in and out of the house, opening entry or garage doors, carrying groceries, and so on?
Of course, people often drive in order to assist them with the functional activities of life – such as shopping. While general impairments may not specifically speak to the question of safety behind the wheel, they do speak to the issue of whether driving is beneficial or necessary. If you or your loved one can no longer perform or engage in other life activities – like shopping – then it may be that driving is no longer helpful. This suggests that it may pose a risk that outweighs any potential benefit.
Additionally, the loss of non-driving-specific abilities indicates a general physical decline any may suggest either that driving-related abilities may soon erode or that further cognitive impairment is on the horizon.[2]
Clearly, being unable to physically control a vehicle, while not an Alzheimer’s-specific problem, may be an indicator that you or your loved one can no longer reliably or safely operate a vehicle.
Perceptual Difficulties
The normal aging process can cause perceptual difficulties. However, Alzheimer’s can exacerbate these issues.
Perceptual difficulties may impact visual-spatial abilities such as being able to judge distance or peripheral vision. Being spooked by shadows or not noticing cars or pedestrians next to you may be a result of diminished perception.
There may also be an inability to see traffic signs, signals, or other drivers (for example, people braking in front of them or merging into the same lane).
Perceptual difficulties may also include a decreasing ability to hear sirens or horns. This poses an obvious danger – especially, though not exclusively, if it is coupled with memory impairments. Forgetting what emergency-vehicle sounds indicate or require in terms of courses of action can lead to accident, injury, or death.
Reasoning Changes
A deviation from a normal route may cause confusion for a person with Alzheimer’s, as they may not be able to react or think through an alternate route. They may also have issues navigating around accidents or construction sites.
A person with this disease, or some other form of cognitive impairment or dementia, may have a reduced reaction time that, in turn, undermines their ability to react to unexpected changes within their route. These include such things as closed roads and bridges, etc., which could potentially lead to accident, and certainly engender confusion.
Deviations and detours can also result in you or your loved one becoming lost.
Concluding Remarks
As difficult as this can be for the afflicted individual, there will come a point where having them behind the wheel of a car or truck will become more of a danger than a benefit.
For more information, please see my companion YouTube video, HERE.
Postscript
In addition to these safety considerations, there may also be legal implications and potential liabilities in regards to a person driving with Alzheimer’s Disease.
While I am not a lawyer or legal expert, I do have several, relevant resources available on AlzheimersProof.com.
[1] Of course, some persons may have lifelong afflictions or disabilities. These will have to be factored in as well. Doing so is beyond the scope of this article. Consult a healthcare or medical professional for personal evaluations or recommendations.
One of the major challenges in caring for someone who has Alzheimer’s Disease, or some other form of dementia, is that they are often prone to “elopement.” Of course, in the context of long-term care, elopement has nothing to do with illicit or surreptitious marriage. It has to do with a cognitively impaired person leaving the safety of the care environment without supervision.
This problem can be extremely vexing for the caregiver and perilous for the Alzheimer’s sufferer. I know this firsthand. On one memorable occasion, my dad was returned to his home by a police officer after he had been found wandering along a busy road in our city. During a snowstorm.
However, I was able to hinder my dad from wandering with an ingenious little gadget. In this article, I’m going to explain how to install that device – a door blocker called the “Defender.”[1] I have installed several of these blockers: one in an apartment, and a couple of them in a townhouse. I absolutely love these products. And I think that you might, too.
Introduction
What’s the Function of the ‘Defender’?
Knowing your loved one can open doors and leave the care environment without you or a caretaker in tow – or even realizing your charge is gone – is a terrifying proposition. Memory and reasoning deficits raise the possibility that he or she could become disoriented and lost, or even injured or worse.
From the perspective of long-term home care, then, the main benefit of these locks is to prevent your loved one from eloping. The devices are inexpensive, and the contemplated modification may be performed relatively easily.
This sort of change is part of what I mean by “Alzheimer’s proofing” your home environment. (This is a concept that I describe more fully HERE.) Under this way of using the phrase, it is a close cousin to childproofing a house as expectant parents would do in preparation for the arrival of a newborn.
Devices Double as Theft Deterrents
These door blockers can deter Alzheimer’s sufferers, or other cognitively disabled persons, from opening exit doors, leaving the care environment, and potentially putting themselves in harm’s way.
But it is worth noting that this particular use – keeping someone inside the house – is a bit of a departure from the product’s stated purpose.
This style of door lock has been designed and marketed as a security device and theft deterrent. When properly installed on an entrance door, the lock helps to prevent forcible entry into a house. It essentially fortifies the door so that even if a thief has jimmied it, or defeated its deadbolt and locking mechanisms, the door blocker will enable the door to remain in a closed position.
So, beyond the standpoint of Alzheimer’s proofing, it will add another layer of security to your home.
Can Your Alzheimer’s-Afflicted Loved One Defeat the Blocker?
As stated, the Defender is intended to be set into a locked position inside the home in order to reduce the probability of forcible entry should an intruder attempt to gain access to the interior of your house.
Given this, it has been designed to be locked and unlocked by normal-functioning adults. Therefore, it is possible for a cognitively impaired person to operate the latch. However, to do so he or she would have to have a number of cognitive and physical abilities. A rough-and-ready enumeration of these might look the following.
Cognitive Abilities Plausibly Needed to Defeat the Blocker:
The ability to notice the device
The capability to identify its function
The capacity to understand or the resourcefulness to determine the correct way to unlock it once
The motor skill and dexterity required to execute the unlocking action
The memory power to remember how to defeat it on subsequent encounters
I’m certainly no medical or psychological expert. But, the likelihood that a cognitively impaired individual would possess this collection of abilities seems to me to be somewhat low. More guardedly, I suppose that I would venture the opinion that the probability is low at least once your loved is sufficiently advanced in his or her dementia to be a serious elopement risk.
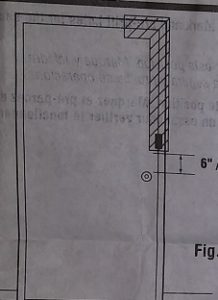
Often, if it is positioned high enough on the door – or if it is camouflaged – your loved one may not even recognize that the door blocker has been installed. Of course, this is because Alzheimer’s tends to diminish perception. In the case of my dad, for instance, I don’t believe he noticed that the thing was even there.
Additionally, a high-up position might hinder the door-opening ability of a senior adult in general – quite apart from any dementia – for example if he or she has joint or mobility issues.
Moreover, the door blocker requires an additional motion, outside of those used to open doors in the usual way, that may frustrate a person with a cognitive deficit and prevent them from eloping from the home.
WARNING!
I should, however, inject an important word of caution.
These door blockers may hinder your and your loved one’s abilities to exit the house in the event of a fire or other emergency. If you’re going to use these products as a deterrent to help prevent elopement of a loved one from the residence, you may want to ensure the blocker is activated only during the time periods where your loved one is at the highest risk of vacating the premises without you noticing.
Of course, from a theft-deterrence perspective, it is appealing to have the latch activated throughout the night or during whatever intervals occupants of the house wish to lower the likelihood of intrusion.[2]
Disclaimer:
I cannot advise you as to the appropriateness of any particular course of action for your application. Furthermore, I cannot be sure, and do not warrant, that the device will be effective for you – for any purpose whatsoever. This information is presented as-is, for general or entertainment purposes only. Whatever use you put this information to is entirely your own responsibility. No one at or affiliated or associated with AlzheimersProof.com assumes any liability for how you may implement or not implement any of the ideas described in on this website or in any companion videos.
Be aware of where and under what circumstances you are installing these blockers. The upshot is that I am certainly not guaranteeing that these devices or installation methods will be successful or safe for your individual or family situation.
I can only state that these blockers were a tremendous help for me and my family when caring for my Alzheimer’s-afflicted dad.
My Installation Procedure
‘Unboxing’ & Collecting Required Tools
‘Defender’ Installation Instructions
Upon opening the Defender’s packaging, you will find several items. These include:
The door blocker device itself;
Instructions;
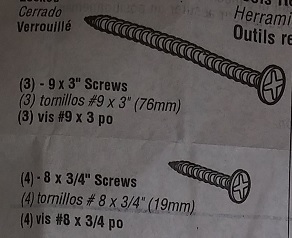
3 large wood screws;
4 smaller metal screws;
Tools
The main tools needed include:
A drill (this could be theoretically be corded or cordless; mine was the latter)
1/8-inch drill bit
Philip’s screwdriver
Optional (& Possibly Necessary) Tools
Wood chisel (if there is insufficient space in between the door and door jamb to accommodate the blocker)
Hammer (to use the chisel, if one is needed)
Center Punch (to tap a small “pilot” for the drill bit)
Tape Measure (to assist in positioning the blocker on the door with respect to the other locking hardware – such as doorknobs and deadbolts)
Safety Equipment
Safety goggles
Positioning the Blocker
You may want to begin by determining where you want to place the Defender door blocker. The instructions suggest that it be installed at least 6 inches above the door handle and deadbolt.
As suggested above, it may be beneficial to install this blocker a bit higher than this. In fact, there is an “L-shaped” area on the door within which the manufacturer recommends placing the Defender.
Inverted ‘L’-Shaped Install Location
While determining where to install the blocker, place the blocker in the locked position. While in this fully closed position, slide the plate between the door frame and door with the black pad against the door.
This will allow you to get a good look at everything, and to reposition the blocker is desired or necessary.
**Be mindful of any electrical outlets nearby as there may be wiring within the walls near where you may be drilling. Additionally, look at surrounding door hardware, molding, key hooks, or other things that might interfere with your ability to operate the blocker and allow it to swing fully from locked to unlocked positions, and back again.
Actual Installation Steps
Step One
Once you have determined where you want to place the door blocker, use a pencil to mark the placement of the center screw within the door frame.
Step Two
Use your drill and 1/8-inch drill bit to make a hole where the center screw will be placed.
Step Three
Place the door blocker plate back against the door frame, allowing the recently drilled hole drilled to be visible in the center-hole of the plate.
Step Four
Drive the center screw into the door frame allowing the blocker plate to be provisionally positioned. The center hole is oval shaped and allows for the back-and-forth movement of the device in order to ensure that it is tight enough against the door to perform its function, but not so tight that it prevents you from latching and unlatching it.
Step Five
Test for the appropriate and desired fit. Before fully securing the door blocker, close the door and test the blocker in the locked position to ensure the placement is optimal. If the lock is difficult to engage or disengage, the placement of the plate may need to be adjusted slightly for proper operation of the device. In this case, you would simply loosen (but not remove) the center screw, move the blocker, and re-tighten the screw.
Step Six
Once the positioning has been established, ensure that the center screw is fully tightened – but not over-torqued. (You don’t want to strip the head or threads.)
Longer Wood Screws & Shorter Metal Screws
Then, drive in the remaining three (3) screws – large screws for a wooden door frame; small screws for metal – into the remaining holes present on the door blocker plate to firmly secure the blocker.
Congratulations!
Your Defender door blocker has now been successfully installed!
‘Defender’ in Position
If you need an additional assist, or a bit more in the way of visual aids, never fear. For a demonstration of the operation of the lock, or for a video tutorial on the installation procedure, please view my companion YouTube video: Alzheimer’s Elopement & Access Control: Install the Defender Door Lock.
Thank you for reading! I wish you all the best trying to deal with elopement risk.
Notes:
[1] The “Defender” appears to me to be an off-brand version of a different door blocker known as the “Door Guardian.” I also have the Door Guardian and will walk through its – nearly identical – installation procedure in a subsequent post.
[2] Note that there is no “key” and that the device is not designed to be unlocked from the outside. It is supposed to be activated and deactivated from within the area being secured.